

Development of a Mouse Model of Metabolic Syndrome, Pulmonary Hypertension, and Heart Failure with Preserved Ejection Fraction
- PMID: 28118022
- PMCID: PMC5449511
- DOI: 10.1165/rcmb.2016-0177OC
Development of a Mouse Model of Metabolic Syndrome, Pulmonary Hypertension, and Heart Failure with Preserved Ejection Fraction
Abstract
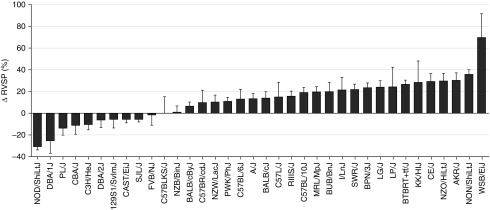
Pulmonary hypertension (PH) associated with heart failure with preserved ejection fraction (PH-HFpEF; World Health Organization Group II) secondary to left ventricular (LV) diastolic dysfunction is the most frequent cause of PH. It is an increasingly recognized clinical complication of the metabolic syndrome. To date, no effective treatment has been identified, and no genetically modifiable mouse model is available for advancing our understanding for PH-HFpEF. To develop a mouse model of PH-HFpEF, we exposed 36 mouse strains to 20 weeks of high-fat diet (HFD), followed by systematic evaluation of right ventricular (RV) and LV pressure-volume analysis. The HFD induces obesity, glucose intolerance, insulin resistance, hyperlipidemia, as well as PH, in susceptible strains. We observed that certain mouse strains, such as AKR/J, NON/shiLtJ, and WSB/EiJ, developed hemodynamic signs of PH-HFpEF. Of the strains that develop PH-HFpEF, we selected AKR/J for further model validation, as it is known to be prone to HFD-induced metabolic syndrome and had low variability in hemodynamics. HFD-treated AKR/J mice demonstrate reproducibly higher RV systolic pressure compared with mice fed with regular diet, along with increased LV end-diastolic pressure, both RV and LV hypertrophy, glucose intolerance, and elevated HbA1c levels. Time course assessments showed that HFD significantly increased body weight, RV systolic pressure, LV end-diastolic pressure, biventricular hypertrophy, and HbA1c throughout the treatment period. Moreover, we also identified and validated 129S1/SvlmJ as a resistant mouse strain to HFD-induced PH-HFpEF. These studies validate an HFD/AKR/J mouse model of PH-HFpEF, which may offer a new avenue for testing potential mechanisms and treatments for this disease.
Keywords: AKR/J; group 2 pulmonary hypertension; metabolic syndrome; pulmonary hypertension; pulmonary hypertension–heart failure with preserved ejection fraction.
Figures




References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 s) uppl:S43–S54. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–327. - PubMed
-
- Damy T, Goode KM, Kallvikbacka-Bennett A, Lewinter C, Hobkirk J, Nikitin NP, Dubois-Randé JL, Hittinger L, Clark AL, Cleland JG. Determinants and prognostic value of pulmonary arterial pressure in patients with chronic heart failure. Eur Heart J. 2010;31:2280–2290. - PubMed
-
- Delgado JF, Conde E, Sánchez V, López-Ríos F, Gómez-Sánchez MA, Escribano P, Sotelo T, Gómez de la Cámara A, Cortina J, de la Calzada CS. Pulmonary vascular remodeling in pulmonary hypertension due to chronic heart failure. Eur J Heart Fail. 2005;7:1011–1016. - PubMed
-
- Leung CC, Moondra V, Catherwood E, Andrus BW. Prevalence and risk factors of pulmonary hypertension in patients with elevated pulmonary venous pressure and preserved ejection fraction. Am J Cardiol. 2010;106:284–286. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
