

Is the outcome at surgery different when flat epithelial atypia and lobular neoplasia are found in association at biopsy?
- PMID: 28118035
- PMCID: PMC5605065
- DOI: 10.1259/bjr.20160750
Is the outcome at surgery different when flat epithelial atypia and lobular neoplasia are found in association at biopsy?
Abstract
Objective: To assess the impact on the final outcome at surgery of flat epithelial atypia (FEA) when found concomitantly with lobular neoplasia (LN) in biopsy specimens compared with pure biopsy-proven FEA.
Methods: The approval from the institutional review board of the CHUM (Centre Hospitalier Universitaire de Montréal) was obtained. A retrospective review of our database between 2009 and 2013 identified 81 females (mean age 54 years, range 38-90 years) with 81 FEA biopsy-proven lesions. These were pure or associated with LN only in 59/81 (73%) and 22/81 (27%) cases, respectively. Overall, 57/81 (70%) patients underwent surgery and 24/81 (30%) patients underwent mammographic surveillance with a mean follow-up of 36 months.
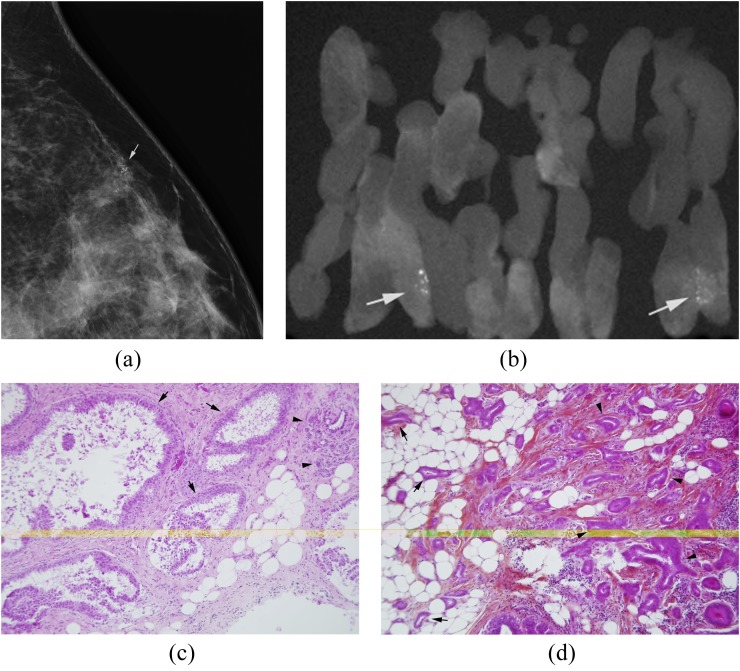
Results: FEA presented more often as microcalcifications in 68/81 (84%) patients and were mostly amorphous in 49/68 (72%). After excluding radio pathologically discordant cases, pure FEA proved to be malignant at surgery in 1/41 (2%; 95% confidence interval 0.06-12.9). There was no statistically significant difference in the upgrade to malignancy whether FEA lesions were pure or associated to LN at biopsy (p = 0.4245); however, when paired in biopsy specimens, these lesions were more frequently associated with atypical ductal hyperplasia (ADH) at surgery than with pure FEA (p = 0.012).
Conclusion: Our results show a 2% upgrade rate to malignancy of pure FEA lesions. When FEA is found in association with LN at biopsy, surgical excision yields more frequently ADH than pure FEA thus warranting close surveillance or even surgical excision. Advances in knowledge: The association of LN with FEA at biopsy was more frequently associated with ADH at surgery than with pure FEA. If a biopsy-proven FEA lesion is deemed concordant with the imaging finding, when paired with LN at biopsy, careful surveillance or even surgical excision is suggested.
Figures
References
-
- Abdel-Fatah TM, Powe DG, Hodi Z, Lee AH, Reis-Filho JS, Ellis IO. High frequency of coexistence of columnar cell lesions, lobular neoplasia, and low grade ductal carcinoma in situ with invasive tubular carcinoma and invasive lobular carcinoma. Am J Surg Pathol 2007; 31: 417–26. - PubMed
-
- Khoumais NA, Scaranelo AM, Moshonov H, Kulkarni SR, Miller N, McCready DR, et al. Incidence of breast cancer in patients with pure flat epithelial atypia diagnosed at core-needle biopsy of the breast. Ann Surg Oncol 2013; 20: 133–8. doi: https://doi.org/10.1245/s10434-012-2591-0 - DOI - PubMed
-
- Schnitt SJ, Vincent-Salomon A. Columnar cell lesions of the breast. Adv Anat Pathol 2003; 10: 113–24. doi: https://doi.org/10.1097/00125480-200305000-00001 - DOI - PubMed
-
- Lerwill MF. Flat epithelial atypia of the breast. Arch Pathol Lab Med 2008; 132: 615–21. doi: https://doi.org/10.1043/1543-2165(2008)132[615:FEAOTB]2.0.CO;2 - DOI - PubMed
-
- Solorzano S, Mesurolle B, Omeroglu A, El Khoury M, Kao E, Aldis A, et al. Flat epithelial atypia of the breast: pathological-radiological correlation. AJR Am J Roentgenol 2011; 197: 740–6. doi: https://doi.org/10.2214/AJR.10.5265 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
