

Clinical and Serologic Features in Patients With Incomplete Lupus Classification Versus Systemic Lupus Erythematosus Patients and Controls
- PMID: 28118528
- PMCID: PMC5524597
- DOI: 10.1002/acr.23201
Clinical and Serologic Features in Patients With Incomplete Lupus Classification Versus Systemic Lupus Erythematosus Patients and Controls
Abstract
Objective: Incomplete lupus erythematosus (ILE) involves clinical and/or serologic manifestations consistent with but insufficient for systemic lupus erythematosus (SLE) classification. Because the nature of ILE is poorly understood and no treatment recommendations exist, we examined the clinical manifestations, medication history, and immunologic features in a diverse collection of ILE and SLE patients.
Methods: Medical records of subjects enrolled in the Lupus Family Registry and Repository were reviewed for medication history and American College of Rheumatology (ACR) classification criteria to identify ILE patients (3 ACR criteria; n = 440) and SLE patients (≥4 ACR criteria; n = 3,397). Participants completed the Connective Tissue Disease Screening Questionnaire. Anticardiolipin and plasma B lymphocyte stimulator (BLyS) were measured by enzyme-linked immunosorbent assay, antinuclear antibodies (ANAs) by indirect immunofluorescence, and 13 autoantibodies by bead-based assays.
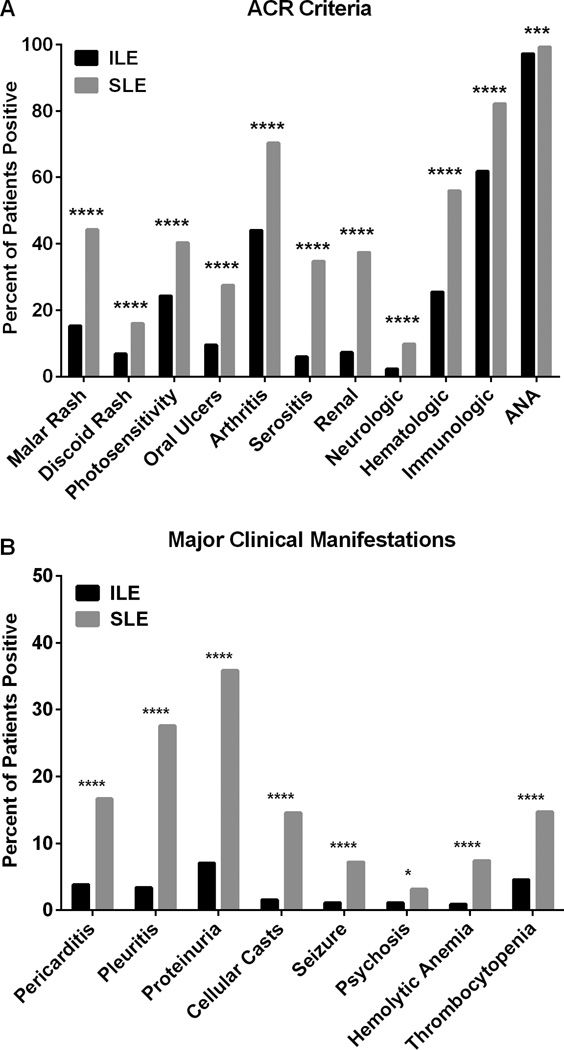
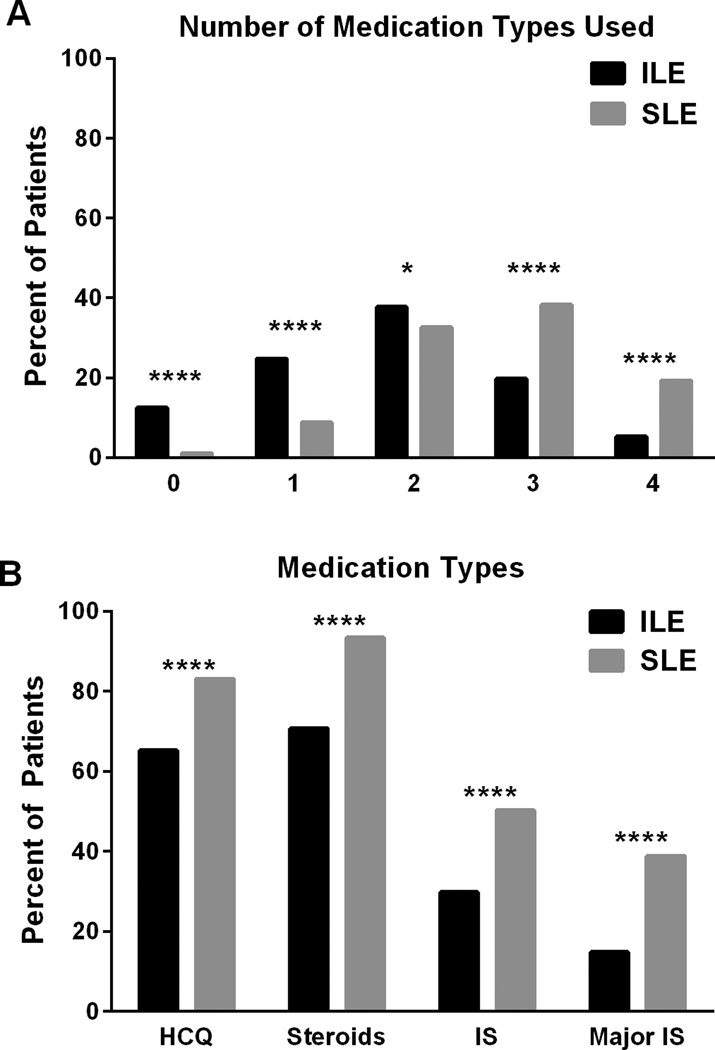
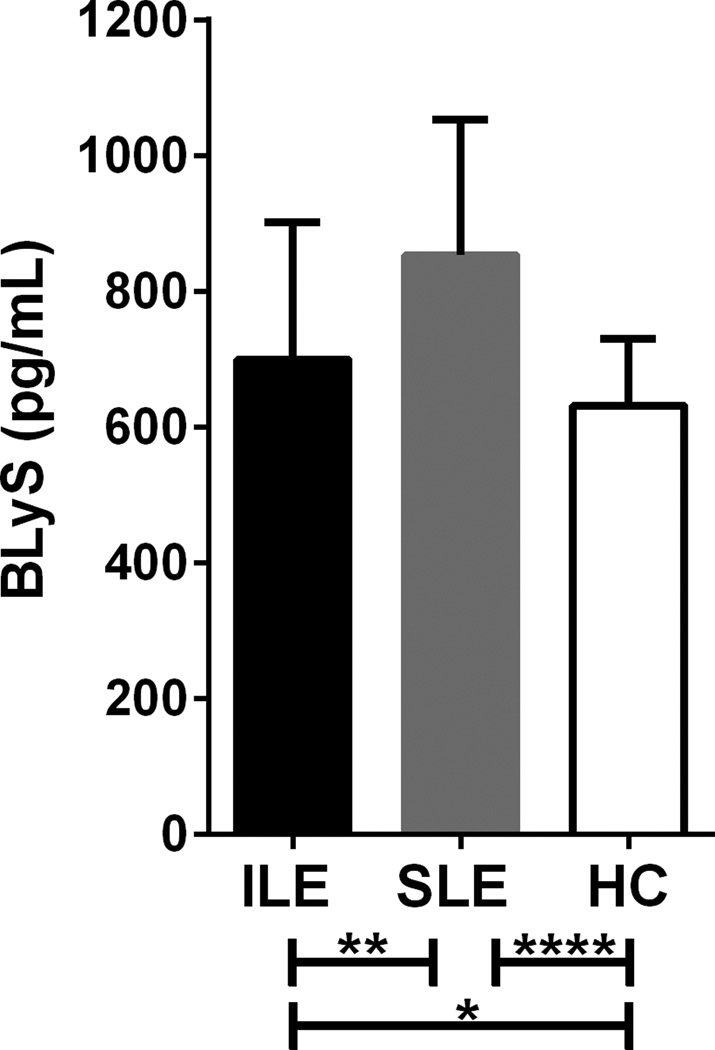
Results: On average, ILE patients were older than SLE patients (46.2 years versus 42.0 years; P < 0.0001), and fewer ILE patients were African American (23.9% versus 32.2%; P < 0.001). ILE patients exhibited fewer autoantibody specificities than SLE patients (1.3 versus 2.6; P < 0.0001) and were less likely to have ANA titers ≥1:1,080 (10.5% versus 19.5%; P < 0.0001). BLyS levels were intermediate in ILE patients (controls < ILE; P = 0.016; ILE < SLE; P = 0.008). Pericarditis, renal, or neurologic manifestations occurred in 12.5% of ILE patients and were associated with non-European American race/ethnicity (P = 0.012). Hydroxychloroquine use increased over time, but was less frequent in ILE than SLE patients (65.2% versus 83.1%; P < 0.0001).
Conclusion: Although usually characterized by milder symptoms, ILE manifestations may require immunomodulatory treatments. Longitudinal studies are necessary to understand how ILE affects organ damage and future SLE risk, and to delineate molecular pathways unique to ILE.
© 2017, American College of Rheumatology.
Conflict of interest statement
All other authors declare no conflicts of interest.
Figures
Comment in
-
How Do We Classify "Incomplete Lupus?".Arthritis Care Res (Hoboken). 2017 Dec;69(12):1777-1779. doi: 10.1002/acr.23196. Arthritis Care Res (Hoboken). 2017. PMID: 28118516 No abstract available.
References
-
- Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982;25(11):1271–1277. - PubMed
-
- Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. - PubMed
-
- Greer JM, Panush RS. INcomplete lupus erythematosus. Arch Int Med. 1989;149(11):2473–2476. - PubMed
-
- Vila L, Mayor A, Valent A, Garc M, Vila S. Clinical outcome and predictors of disease evolution in patients with incomplete lupus erythematosus. Lupus. 2000;9(2):110–115. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U54 GM104938/GM/NIGMS NIH HHS/United States
- U19 AI082714/AI/NIAID NIH HHS/United States
- P30 GM103510/GM/NIGMS NIH HHS/United States
- P30 AR053483/AR/NIAMS NIH HHS/United States
- R01 DK107502/DK/NIDDK NIH HHS/United States
- R24 HL105333/HL/NHLBI NIH HHS/United States
- R37 AI024717/AI/NIAID NIH HHS/United States
- U01 AI101934/AI/NIAID NIH HHS/United States
- R01 AI024717/AI/NIAID NIH HHS/United States
- U01 HG008666/HG/NHGRI NIH HHS/United States
- P30 AR070549/AR/NIAMS NIH HHS/United States
- I01 BX001834/BX/BLRD VA/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
