

Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival
- PMID: 28118660
- PMCID: PMC6056890
- DOI: 10.1001/jama.2016.20165
Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival
Abstract
Importance: Tracheal intubation is common during adult in-hospital cardiac arrest, but little is known about the association between tracheal intubation and survival in this setting.
Objective: To determine whether tracheal intubation during adult in-hospital cardiac arrest is associated with survival to hospital discharge.
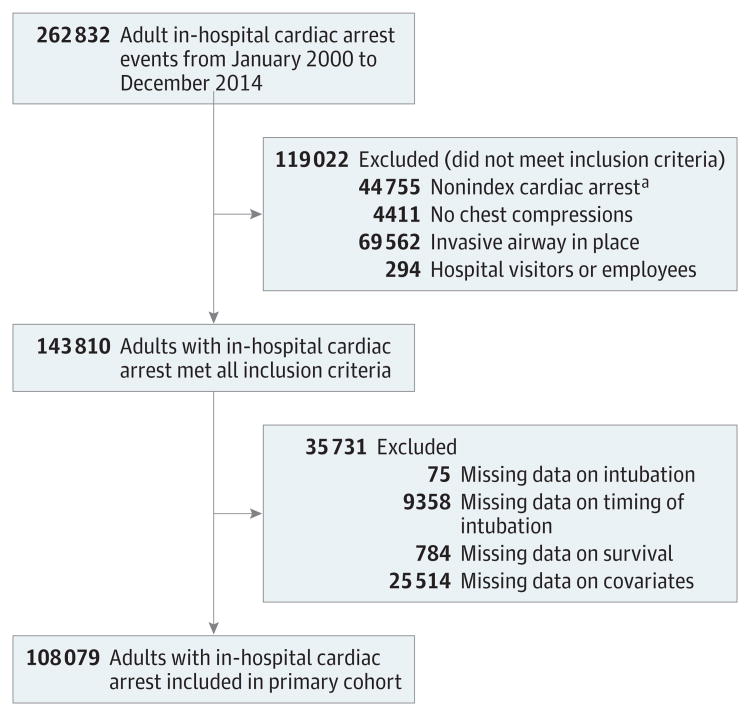
Design, setting, and participants: Observational cohort study of adult patients who had an in-hospital cardiac arrest from January 2000 through December 2014 included in the Get With The Guidelines-Resuscitation registry, a US-based multicenter registry of in-hospital cardiac arrest. Patients who had an invasive airway in place at the time of cardiac arrest were excluded. Patients intubated at any given minute (from 0-15 minutes) were matched with patients at risk of being intubated within the same minute (ie, still receiving resuscitation) based on a time-dependent propensity score calculated from multiple patient, event, and hospital characteristics.
Exposure: Tracheal intubation during cardiac arrest.
Main outcomes and measures: The primary outcome was survival to hospital discharge. Secondary outcomes included return of spontaneous circulation (ROSC) and a good functional outcome. A cerebral performance category score of 1 (mild or no neurological deficit) or 2 (moderate cerebral disability) was considered a good functional outcome.
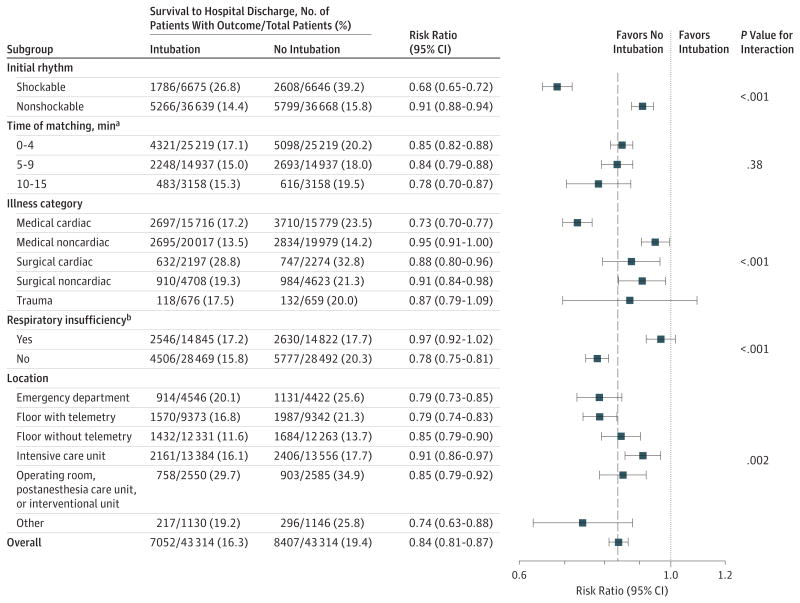
Results: The propensity-matched cohort was selected from 108 079 adult patients at 668 hospitals. The median age was 69 years (interquartile range, 58-79 years), 45 073 patients (42%) were female, and 24 256 patients (22.4%) survived to hospital discharge. Of 71 615 patients (66.3%) who were intubated within the first 15 minutes, 43 314 (60.5%) were matched to a patient not intubated in the same minute. Survival was lower among patients who were intubated compared with those not intubated: 7052 of 43 314 (16.3%) vs 8407 of 43 314 (19.4%), respectively (risk ratio [RR] = 0.84; 95% CI, 0.81-0.87; P < .001). The proportion of patients with ROSC was lower among intubated patients than those not intubated: 25 022 of 43 311 (57.8%) vs 25 685 of 43 310 (59.3%), respectively (RR = 0.97; 95% CI, 0.96-0.99; P < .001). Good functional outcome was also lower among intubated patients than those not intubated: 4439 of 41 868 (10.6%) vs 5672 of 41 733 (13.6%), respectively (RR = 0.78; 95% CI, 0.75-0.81; P < .001). Although differences existed in prespecified subgroup analyses, intubation was not associated with improved outcomes in any subgroup.
Conclusions and relevance: Among adult patients with in-hospital cardiac arrest, initiation of tracheal intubation within any given minute during the first 15 minutes of resuscitation, compared with no intubation during that minute, was associated with decreased survival to hospital discharge. Although the study design does not eliminate the potential for confounding by indication, these findings do not support early tracheal intubation for adult in-hospital cardiac arrest.
Conflict of interest statement
Figures
Comment in
-
Whether to Intubate During Cardiopulmonary Resuscitation: Conventional Wisdom vs Big Data.JAMA. 2017 Feb 7;317(5):477-478. doi: 10.1001/jama.2016.20626. JAMA. 2017. PMID: 28118658 No abstract available.
-
Intubation During In-Hospital Cardiac Arrest.JAMA. 2017 May 16;317(19):2019. doi: 10.1001/jama.2017.4419. JAMA. 2017. PMID: 28510672 No abstract available.
-
The end of the road for early tracheal intubation in cardiac arrest?J Thorac Dis. 2017 Apr;9(4):976-978. doi: 10.21037/jtd.2017.03.162. J Thorac Dis. 2017. PMID: 28523152 Free PMC article. No abstract available.
-
Endotracheal Intubation in Critically III Patients: Direct Laryngoscopy, Complications, and Cardiac Arrest.Am J Respir Crit Care Med. 2018 Jun 15;197(12):1625-1627. doi: 10.1164/rccm.201709-1884RR. Am J Respir Crit Care Med. 2018. PMID: 29624406 No abstract available.
-
In-Hospital Cardiac Arrest: Intubate or Not?J Perianesth Nurs. 2018 Aug;33(4):551-552. doi: 10.1016/j.jopan.2018.06.001. J Perianesth Nurs. 2018. PMID: 30077299 No abstract available.
References
-
- Callaway CW, Soar J, Aibiki M, et al. Advanced Life Support Chapter Collaborators. Part 4: advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015;132(16) suppl 1:S84–S145. - PubMed
-
- Link MS, Berkow LC, Kudenchuk PJ, et al. Part 7: adult advanced cardiovascular life support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18) suppl 2:S444–S464. - PubMed
-
- Soar J, Nolan JP, Böttiger BW, et al. Adult Advanced Life Support Section Collaborators. European Resuscitation Council Guidelines for Resuscitation 2015: section 3: adult advanced life support. Resuscitation. 2015;95:100–147. - PubMed
-
- Hasegawa K, Hiraide A, Chang Y, Brown DF. Association of prehospital advanced airway management with neurologic outcome and survival in patients with out-of-hospital cardiac arrest. JAMA. 2013;309(3):257–266. - PubMed
-
- Fredriksson M, Aune S, Bång A, et al. Cardiac arrest outside and inside hospital in a community: mechanisms behind the differences in outcome and outcome in relation to time of arrest. Am Heart J. 2010;159(5):749–756. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
