

Analysis of clinical factors affecting the rates of fatal pulmonary embolism and bleeding in cancer patients with venous thromboembolism
- PMID: 28119956
- PMCID: PMC5239824
- DOI: 10.1016/j.heliyon.2016.e00229
Analysis of clinical factors affecting the rates of fatal pulmonary embolism and bleeding in cancer patients with venous thromboembolism
Abstract
Background: In cancer patients with symptomatic venous thromboembolism (VTE) (deep-vein thrombosis (DVT) and/or pulmonary embolism (PE)), clinical factors that influence the benefit-risk balance of anticoagulation need to be identified so treatment intensity and duration can be optimally adjusted for the individual patient.
Methods: Using clinical data for cancer patients with VTE obtained from the RIETE registry, we compared how rates of fatal PE and fatal bleeding during and after anticoagulation vary depending on patients' clinical characteristics.
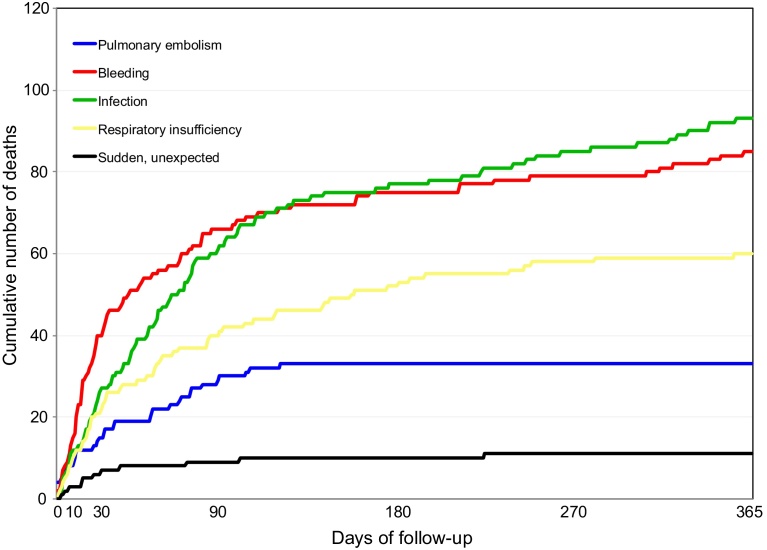
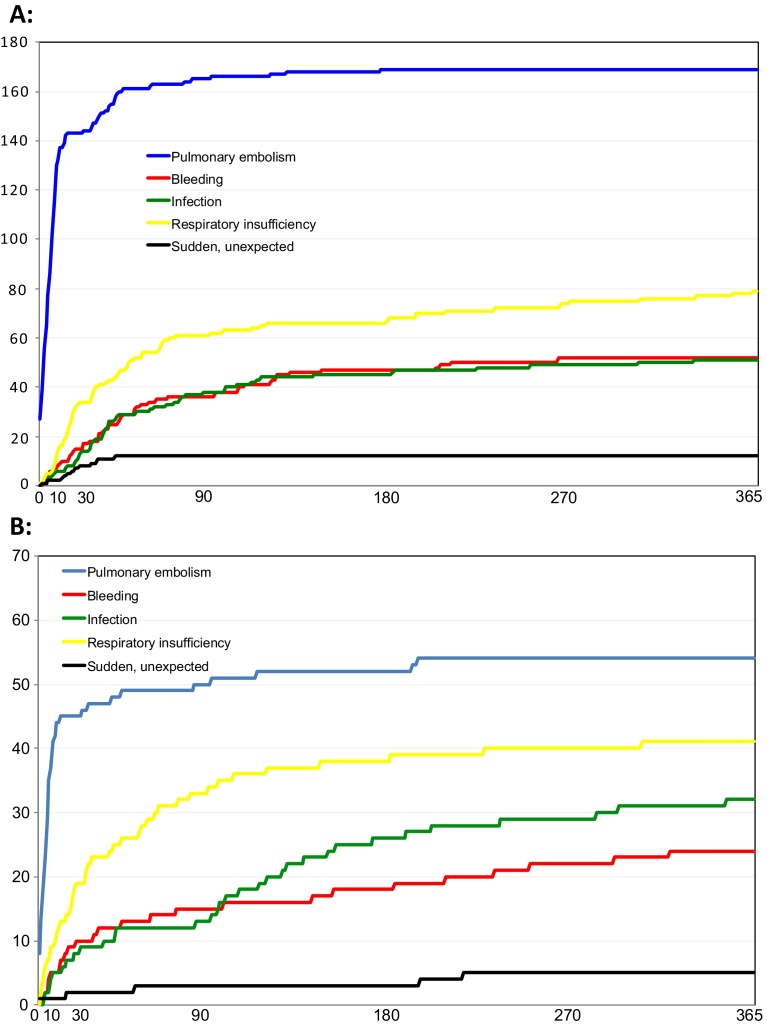
Results: Data were analysed from the 10,962 cancer patients with VTE (5,740 with PE with or without DVT; 5,222 with DVT alone) in RIETE registry as of March 2016. Fatal PE occurred in 2.18% of patients, while fatal bleedings occurred in 1.55%. During the 12 months from initial VTE, fatal PE was the most common cause of death, after disseminating cancer, and bleeding the fourth most common. In patients initially presenting with PE, fatal PE during anticoagulation was 4-fold more frequent than fatal bleeding (204 vs 51 deaths) and occurred mostly during the first month of treatment (196/223, 88%). In patients initially presenting with DVT, fatal PE was 3-fold lower than fatal bleeding during (25 vs 85 deaths) and after anticoagulation treatment (8 vs 37 deaths). During the 12-month follow-up, other characteristics of cancer patients with VTE were identified as more common in fatal cases of PE and/or bleeding than in surviving cases.
Interpretation: Baseline clinical characteristics may determine anticoagulation outcomes in cancer patients with VTE and should be further investigated as possible factors for guiding changes in current practices of anticoagulation, such as adjusting anticoagulation intensity and duration in selected patients.
Keywords: Health Sciences; Medicine.
Figures


References
-
- Kearon C., Akl E.A., Comerota A.J., Prandoni P., Bounameaux H., Goldhaber S.Z. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S–e494S. - PMC - PubMed
-
- Khorana A.A. Cancer-associated thrombosis: updates and controversies. Hematol. Am. Soc. Hematol. Educ. Program. 2012;2012:626–630. - PubMed
-
- Imberti D., Agnelli G., Ageno W., Moia M., Palareti G., Pistelli R. Clinical characteristics and management of cancer-associated acute venous thromboembolism: findings from the MASTER Registry. Haematologica. 2008;93(2):273–278. - PubMed
-
- Guijarro R., de Miguel-Diez J., Jimenez D., Trujillo-Santos J., Otero R., Barba R. Pulmonary embolism, acute coronary syndrome and ischemic stroke in the Spanish National Discharge Database. Eur. J. Intern. Med. 2016;28:65–69. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
