

Impact of rotor temperospatial stability on acute and one-year atrial fibrillation ablation outcomes
- PMID: 28120392
- PMCID: PMC6490561
- DOI: 10.1002/clc.22674
Impact of rotor temperospatial stability on acute and one-year atrial fibrillation ablation outcomes
Abstract
Background: The utility of rotor ablation using commercially available systems as an adjunct to pulmonary vein isolation (PVI) is controversial. Variable results may stem from heterogeneous practice patterns. We investigated whether a prespecified protocol to determine temperospatial rotor stability improved acute and intermediate outcomes following rotor ablation.
Hypothesis: Protocolized rotor mapping and ablation, with prespecified metrics to determine temporal rotor stability prior to ablation, will improve short- and long-term PVI/rotor ablation outcomes.
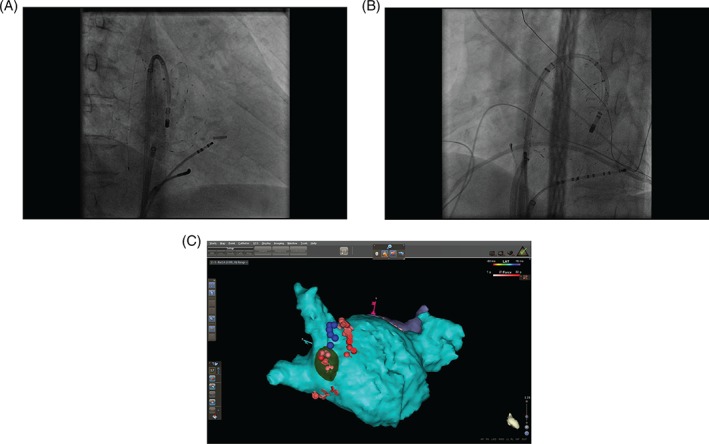
Methods: Patients undergoing PVI plus rotor ablation at Johns Hopkins during 2015 were included. The first cohort underwent rotor mapping and ablation at the operator's discretion, whereas the second cohort underwent protocolized rotor mapping, with ablation limited to temperospatially stable rotors. Both cohorts underwent PVI. Acute results (rotor elimination, atrial fibrillation [AF] termination), procedural data, and 1-year outcomes were assessed.
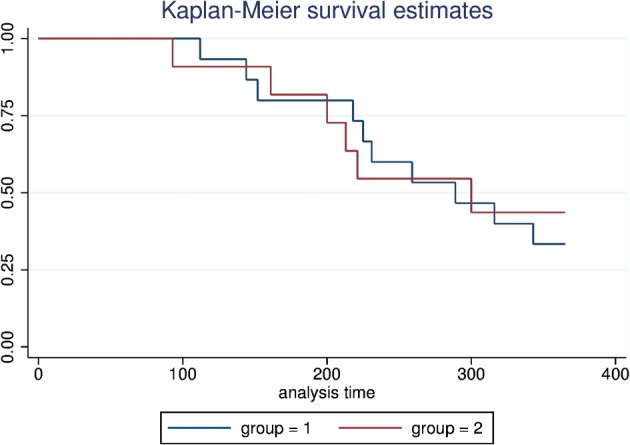
Results: Twenty-seven patients underwent ablation (mean age, 64.4 ± 9 years, male 81.5%, persistent AF 85.2%, long-standing persistent AF 14.8%, mean AF duration 4.4 ± 4 years, repeat cases 51.8%, and mean LA size 4.6 ± 0.8 cm). In the protocolized cohort, rotors were reproducible in 83% (10/12) of cases in at least 1 chamber. Acute rhythm change was achieved in 8/27 (29.6%) patients. Sinus rhythm on presentation (62.5% vs 15.8%, P = 0.03) and higher total targeted rotors (3.8 ± 1.7 vs 2.5 ± 1.0, P = 0.02) predicted acute change. At 12 months, freedom from AF/atrial tachycardia was achieved in 5/15 (33.3%) patients in the first cohort and 5/11 patients in the protocolized cohort (45.5%; P = 0.53 for comparison).
Conclusions: Acute and intermediate results did not change with protocolized mapping designed to identify temperospatially stable rotors. Outcomes at 12 months were similar in both groups.
Keywords: Arrhythmia; Atrial fibrillation; Catheter ablation; Focal impulse and rotor modulation.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Calkins H, Kuck KH, Cappato R, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow‐up, definitions, endpoints, and research trial design. Heart Rhythm. 2012;9:632–696. - PubMed
-
- Weerasooriya R, Khairy P, Litalien J, et al. Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow up? J Am Coll Cardiol. 2011;57:160–166. - PubMed
-
- Narayan SM, Baykaner T, Clopton P, et al. Ablation of rotor and focal sources reduces late recurrence of atrial fibrillation compared with trigger ablation alone: extended follow‐up of the CONFIRM trial (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation). J Am Coll Cardiol. 2014;63:1761–1768. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
