

Long Pentraxin 3 as a Predictive Marker of Mortality in Severe Septic Patients Who Received Successful Early Goal-Directed Therapy
- PMID: 28120568
- PMCID: PMC5290017
- DOI: 10.3349/ymj.2017.58.2.370
Long Pentraxin 3 as a Predictive Marker of Mortality in Severe Septic Patients Who Received Successful Early Goal-Directed Therapy
Abstract
Purpose: Pentraxin 3 (PTX3) has been suggested to be a prognostic marker of mortality in severe sepsis. Currently, there are limited data on biomarkers including PTX3 that can be used to predict mortality in severe sepsis patients who have undergone successful initial resuscitation through early goal-directed therapy (EGDT).
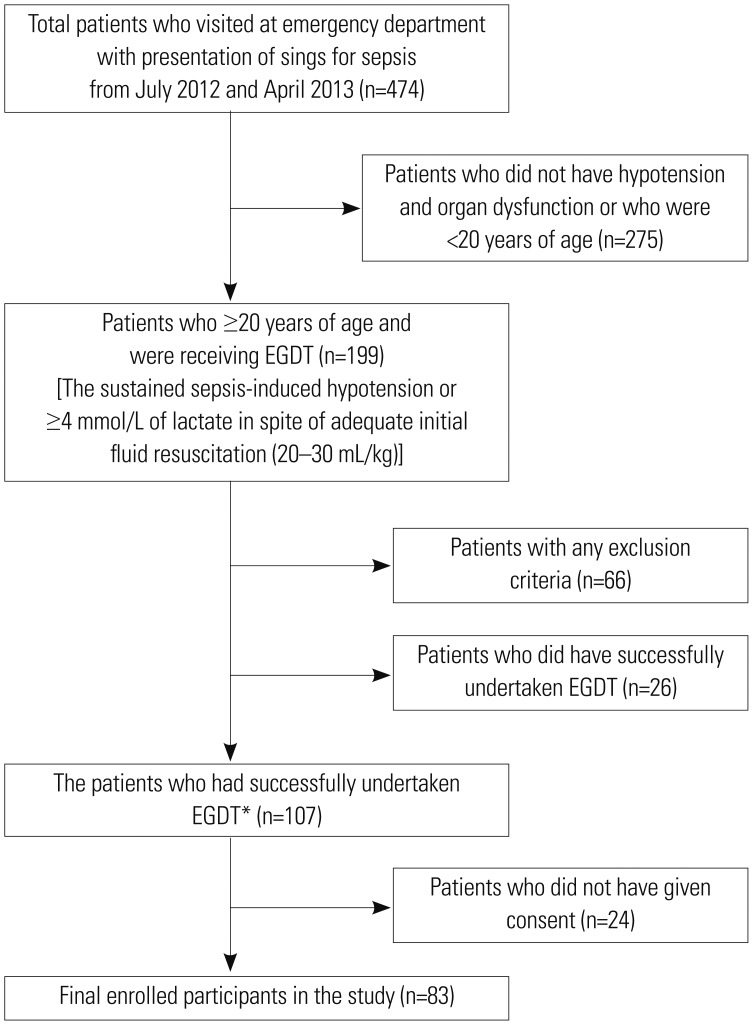
Materials and methods: A prospective cohort study was conducted among 83 severe sepsis patients with fulfillment of all EGDT components and the achievement of final goal. Plasma PTX3 levels were measured by sandwich ELISA on hospital day (HD) 0, 3, and 7. The data for procalcitonin, C-reactive protein and delta neutrophil index were collected by electric medical record. The primary outcome was 28-day all-cause mortality.
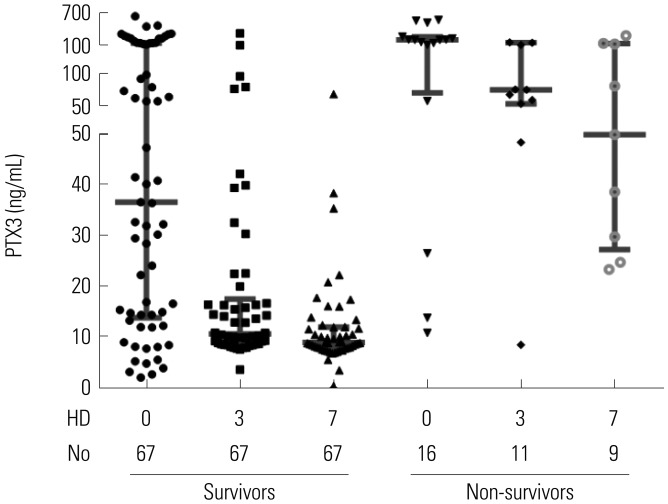
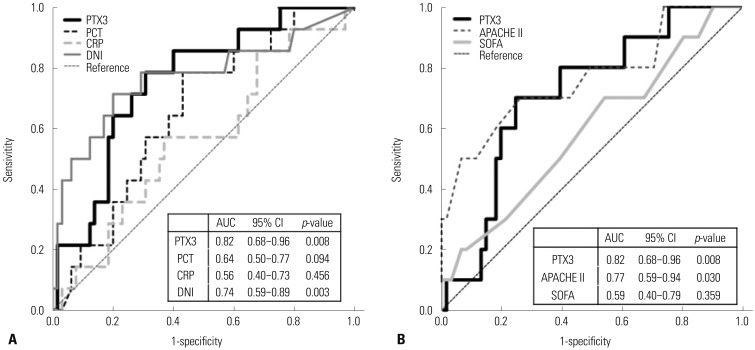
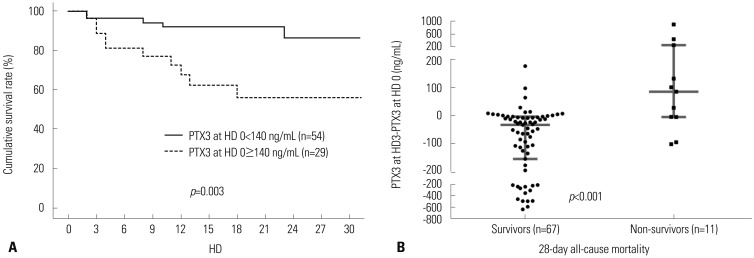
Results: 28-day all-cause mortality was 19.3% and the median (interquartile range) APHCH II score of total patients was 16 (13-19). The non-survivors (n=16) had significantly higher PTX3 level at HD 0 [201.4 (56.9-268.6) ng/mL vs. 36.5 (13.7-145.3) ng/mL, p=0.008]. PTX3 had largest AUC(ROC) value for the prediction of mortality among PTX3, procalcitonin, delta neutrophil index, CRP and APACHE II/SOFA sore at HD 0 [0.819, 95% confidence interval (CI) 0.677-0.961, p=0.008]. The most valid cut-off level of PTX3 at HD 0 was 140.28 ng/mL (sensitivity 66.7%, specificity 73.8%). The PTX3 and procalcitonin at HD 0 showed strong correlation (r=0.675, p<0.001). However, PTX3 at HD 0 was the only independent predictive marker in Cox's proportional hazards model (≥140 ng/mL; hazard rate 7.16, 95% CI 2.46-15.85, p=0.001).
Conclusion: PTX3 at HD 0 could be a powerful predictive biomarker of 28-day all-cause mortality in severe septic patients who have undergone successful EGDT.
Keywords: Pentraxin 3; early-goal directed therapy; mortality; predictive biomarker; severe sepsis.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Bottazzi B, Garlanda C, Cotena A, Moalli F, Jaillon S, Deban L, et al. The long pentraxin PTX3 as a prototypic humoral pattern recognition receptor: interplay with cellular innate immunity. Immunol Rev. 2009;227:9–18. - PubMed
-
- Hasday JD, Bascom R, Costa JJ, Fitzgerald T, Dubin W. Bacterial endotoxin is an active component of cigarette smoke. Chest. 1999;115:829–835. - PubMed
-
- Breviario F, d'Aniello EM, Golay J, Peri G, Bottazzi B, Bairoch A, et al. Interleukin-1-inducible genes in endothelial cells. Cloning of a new gene related to C-reactive protein and serum amyloid P component. J Biol Chem. 1992;267:22190–22197. - PubMed
-
- Introna M, Alles VV, Castellano M, Picardi G, De Gioia L, Bottazzai B, et al. Cloning of mouse PTX3, a new member of the pentraxin gene family expressed at extrahepatic sites. Blood. 1996;87:1862–1872. - PubMed
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
