

The Paley ulnarization of the carpus with ulnar shortening osteotomy for treatment of radial club hand
- PMID: 28120747
- PMCID: PMC5264527
- DOI: 10.1051/sicotj/2016040
The Paley ulnarization of the carpus with ulnar shortening osteotomy for treatment of radial club hand
Abstract
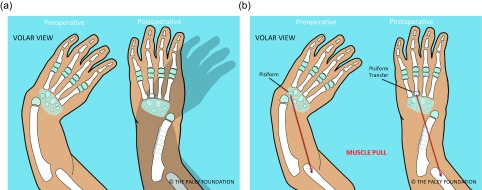
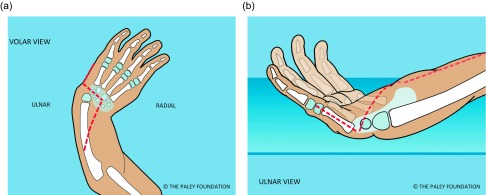
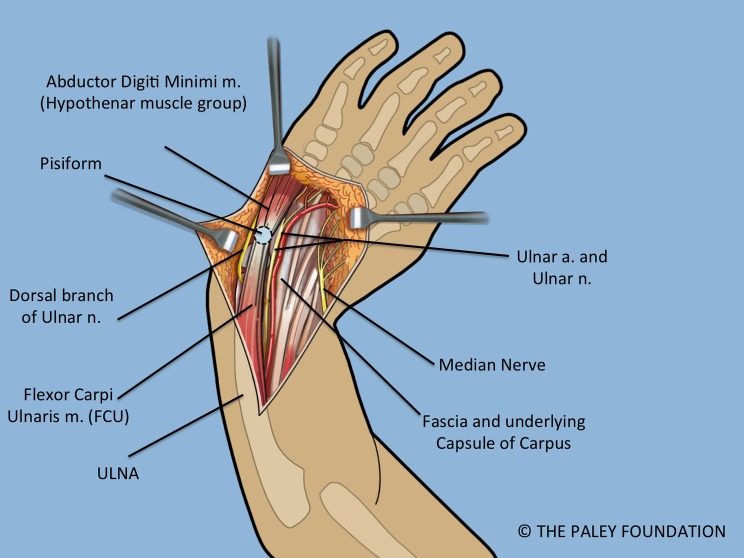
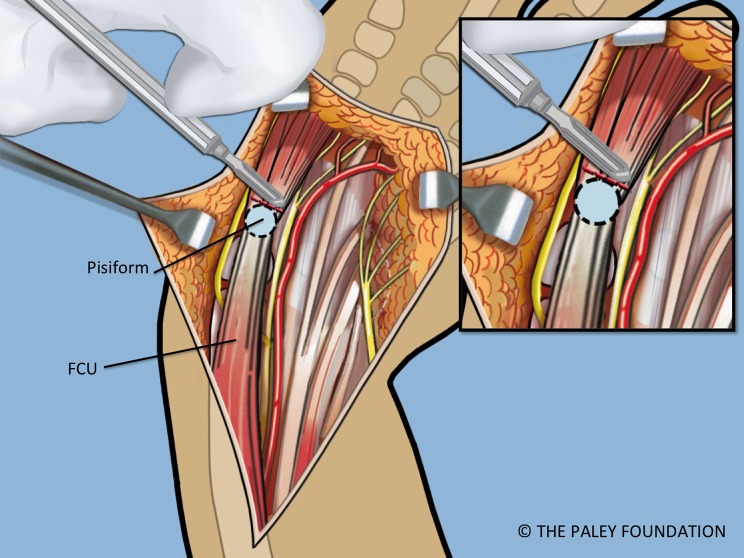
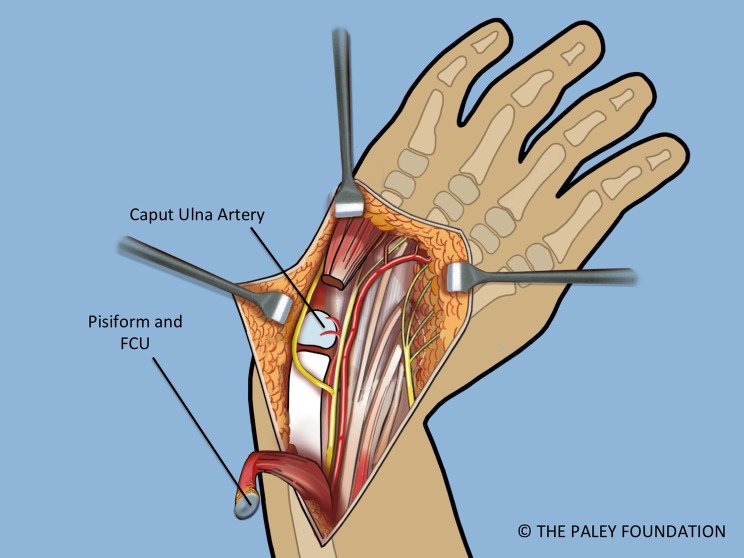
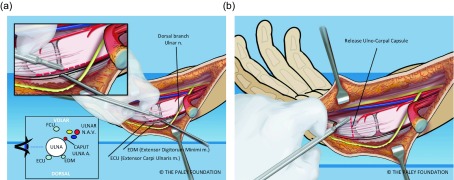
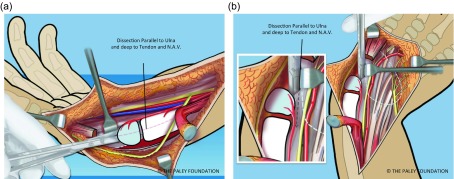
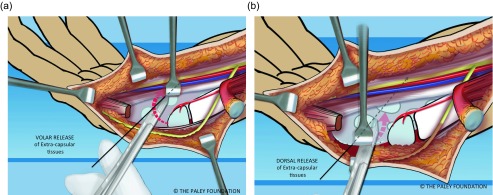
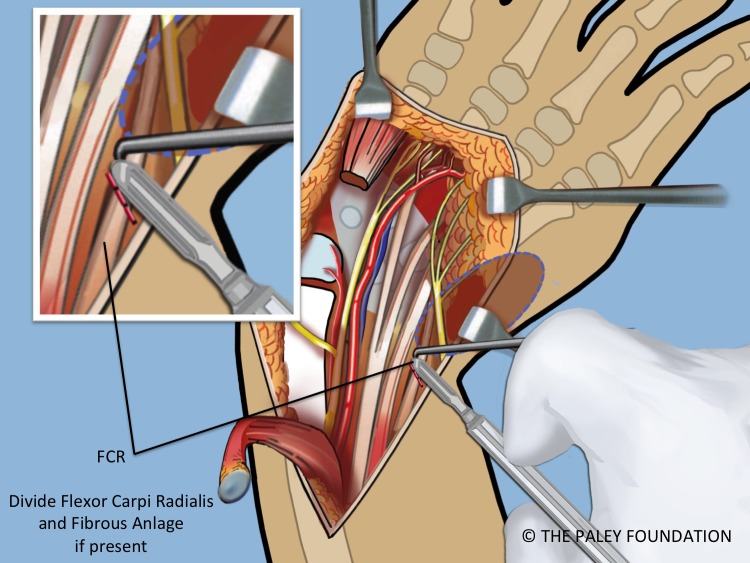
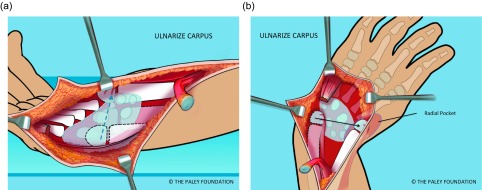
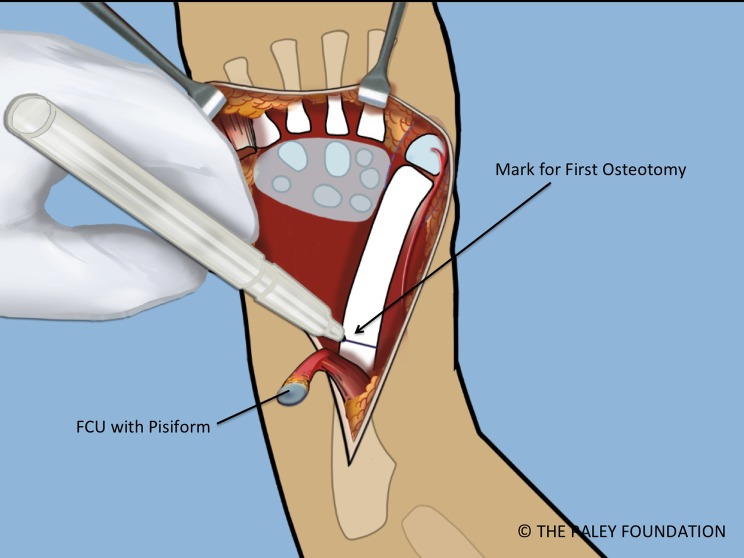
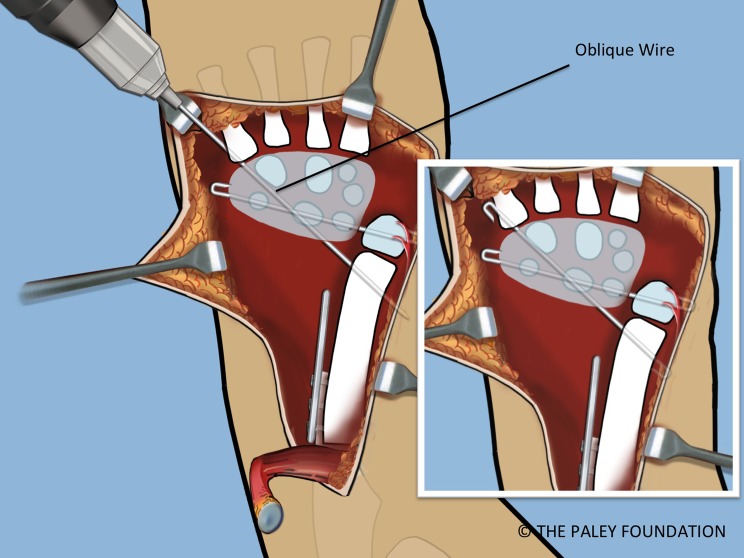
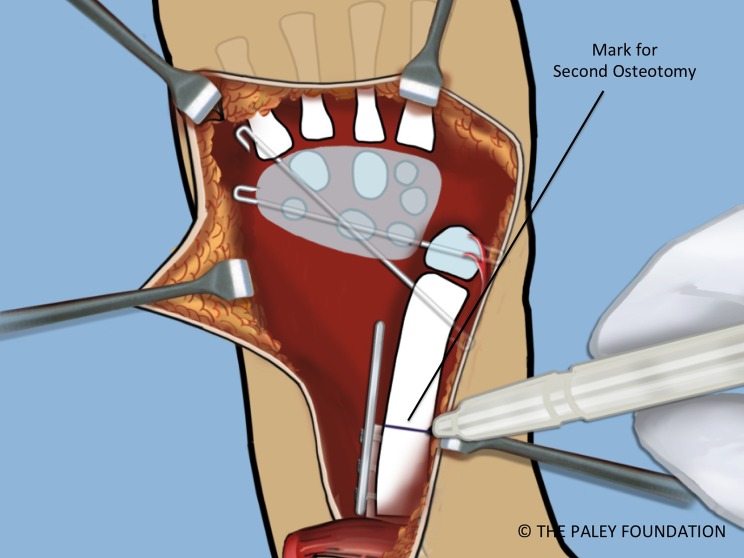
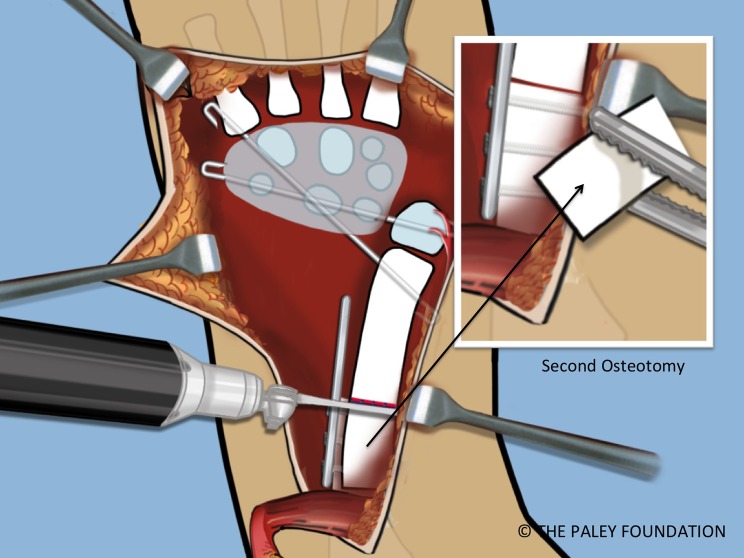
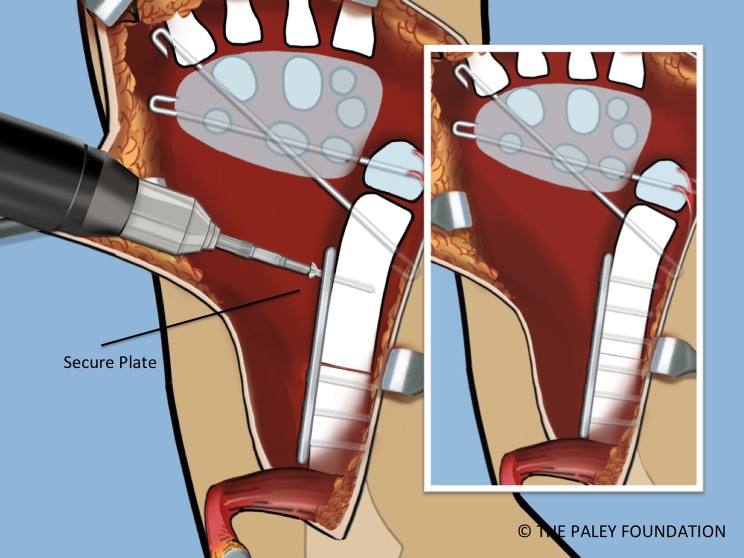
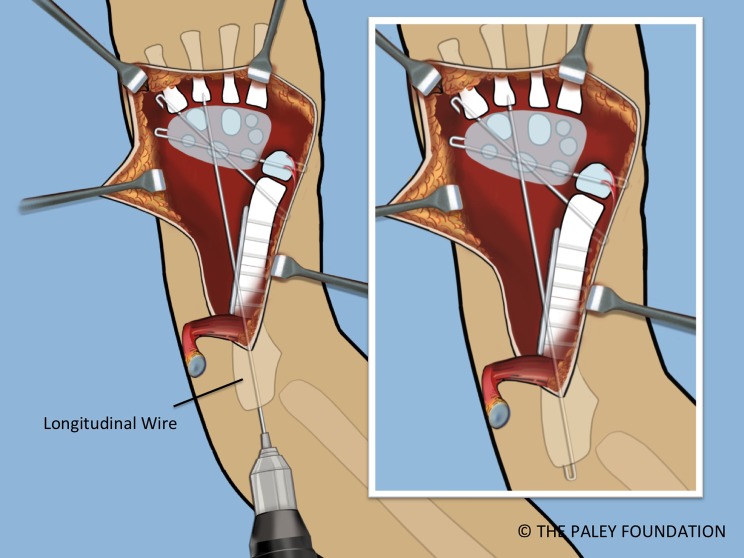
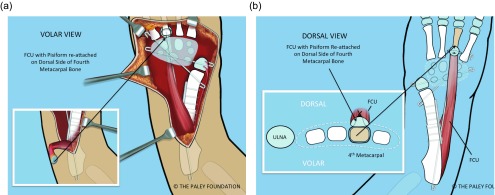
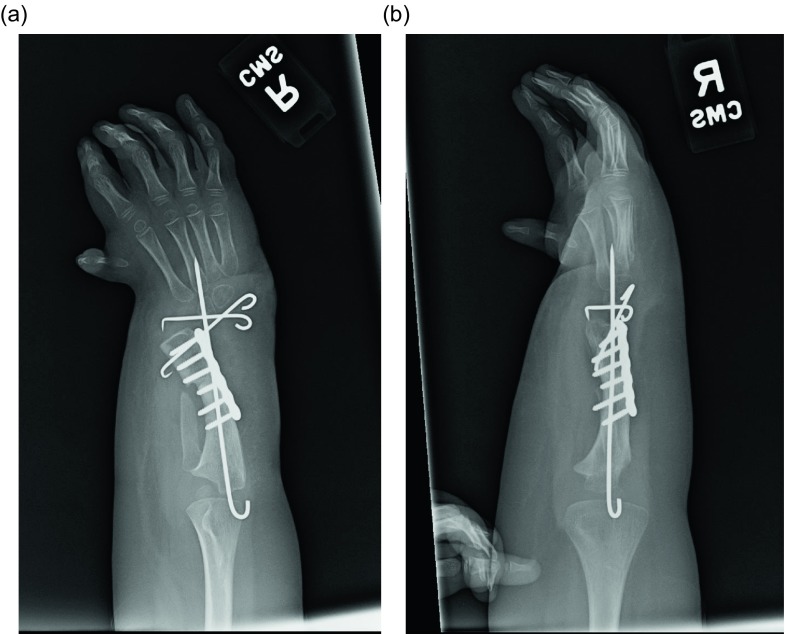
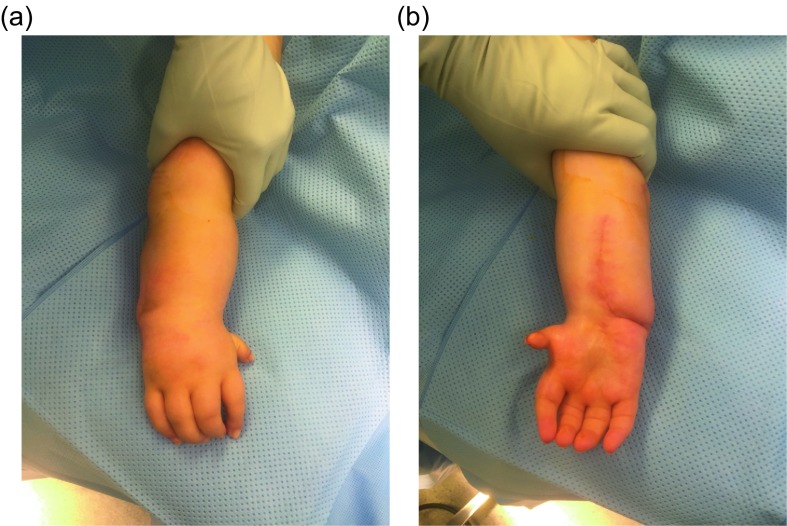
Recurrent deformity from centralization and radialization led to the development in 1999 of a new technique by the author called ulnarization. This method is performed through a volar approach in a vascular and physeal sparing fashion. It biomechanically balances the muscle forces on the wrist by dorsally transferring the flexor carpi ulnaris (FCU) from a deforming to a corrective force. The previous problems of a prominent bump from the ulnar head and ulnar deviation instability were solved by acutely shortening the diaphysis and by temporarily fixing the station of the carpus to the ulnar head at the level of the scaphoid. This is the first report of this modified Paley ulnarization method, which the author considers a significant improvement over his original procedure.
© The Authors, published by EDP Sciences, 2017.
Figures










References
-
- Manske PR (1996) Longitudinal failure of upper-limb formation. Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. J Bone Joint Surg 78A, 1600–1623. - PubMed
-
- Blauth W (1969) On the morphology and therapy of the radial club-hand [in German]. Arch Orthop Unfallchir 65, 97–123. - PubMed
-
- Lamb DW (1974) The treatment of radial club hand: absent radius, aplasia of the radius, hypoplasia of the radius, radial paraxial hemimelia. Hand 4, 22–30. - PubMed
-
- Lamb DW (1977) Radial club hand: a continuing study of sixty-eight patients with one hundred and seventeen club hands. J Bone Joint Surg 59A, 1–13. - PubMed
-
- Watson HK, Beebe RD, Cruz NI (1984) A centralization procedure for radial clubhand. J Hand Surg 9A, 541–547. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources