

Diet and ADHD, Reviewing the Evidence: A Systematic Review of Meta-Analyses of Double-Blind Placebo-Controlled Trials Evaluating the Efficacy of Diet Interventions on the Behavior of Children with ADHD
- PMID: 28121994
- PMCID: PMC5266211
- DOI: 10.1371/journal.pone.0169277
Diet and ADHD, Reviewing the Evidence: A Systematic Review of Meta-Analyses of Double-Blind Placebo-Controlled Trials Evaluating the Efficacy of Diet Interventions on the Behavior of Children with ADHD
Abstract
Introduction: Attention-deficit/hyperactivity disorder (ADHD) is a debilitating mental health problem hampering the child's development. The underlying causes include both genetic and environmental factors and may differ between individuals. The efficacy of diet treatments in ADHD was recently evaluated in three reviews, reporting divergent and confusing conclusions based on heterogeneous studies and subjects. To address this inconsistency we conducted a systematic review of meta-analyses of double-blind placebo-controlled trials evaluating the effect of diet interventions (elimination and supplementation) on ADHD.
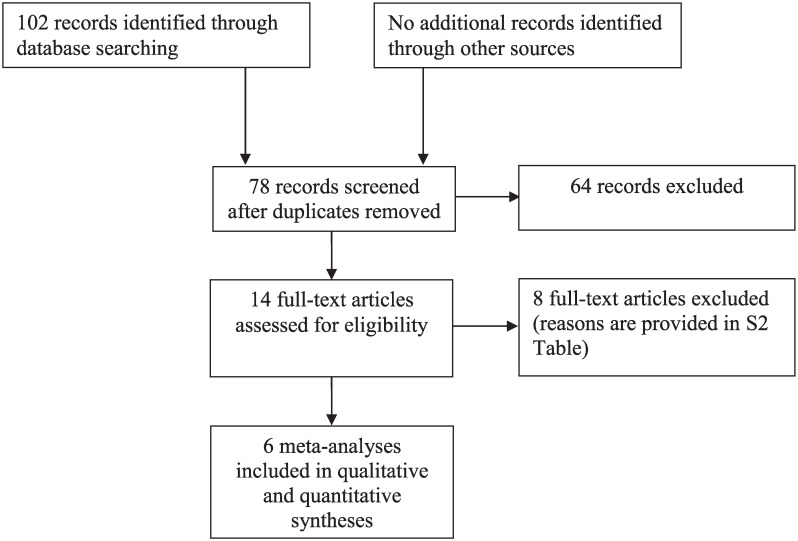
Methods: Our literature search resulted in 14 meta-analyses, six of which confined to double-blind placebo-controlled trials applying homogeneous diet interventions, i.e. artificial food color (AFC) elimination, a few-foods diet (FFD) and poly-unsaturated fatty acid (PUFA) supplementation. Effect sizes (ES) and Confidence intervals (CI) of study outcomes were depicted in a forest plot. I2 was calculated to assess heterogeneity if necessary and additional random effects subgroup meta-regression was conducted if substantial heterogeneity was present.
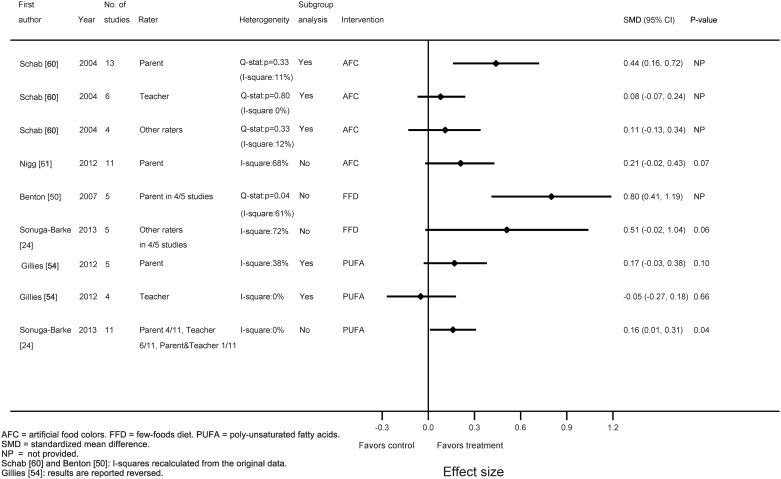
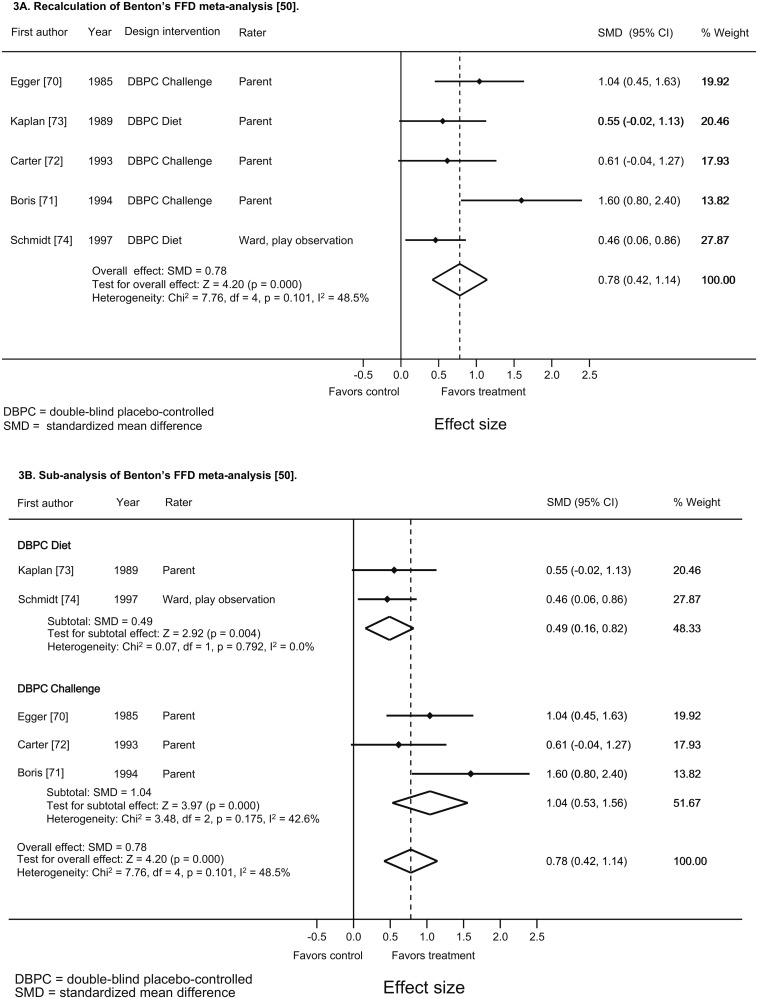
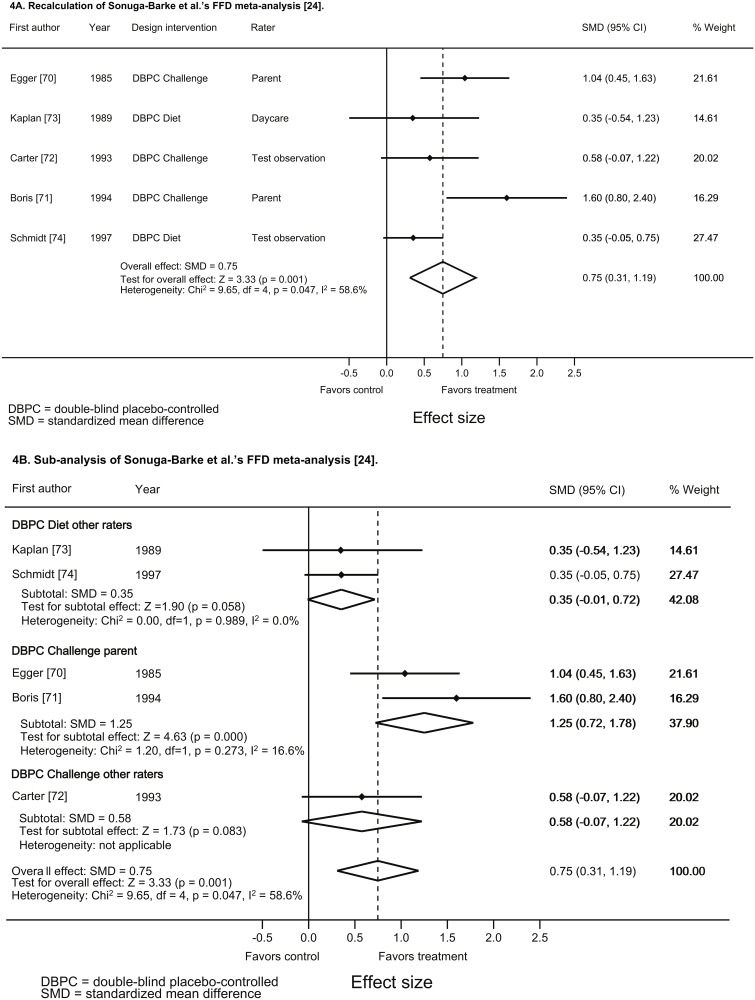
Results: The AFC ESs were 0.44 (95% CI: 0.16-0.72, I2 = 11%) and 0.21 (95% CI: -0.02-0.43, I2 = 68%) [parent ratings], 0.08 (95% CI: -0.07-0.24, I2 = 0%) [teacher ratings] and 0.11 (95% CI: -0.13-0.34, I2 = 12%) [observer ratings]. The FFD ESs were 0.80 (95% CI: 0.41-1.19, I2 = 61%) [parent ratings] and 0.51 (95% CI: -0.02-1.04, I2 = 72%) [other ratings], while the PUFA ESs were 0.17 (95% CI: -0.03-0.38, I2 = 38%) [parent ratings], -0.05 (95% CI: -0.27-0.18, I2 = 0%) [teacher ratings] and 0.16 (95% CI: 0.01-0.31, I2 = 0%) [parent and teacher ratings]. Three meta-analyses (two FFD and one AFC) resulted in high I2 without presenting subgroup results. The FFD meta-analyses provided sufficient data to perform subgroup analyses on intervention type, resulting in a decrease of heterogeneity to 0% (diet design) and 37.8% (challenge design).
Conclusion: Considering the small average ESs PUFA supplementation is unlikely to provide a tangible contribution to ADHD treatment, while further research is required for AFC elimination before advising this intervention as ADHD treatment. The average FFD ES is substantial, offering treatment opportunities in subgroups of children with ADHD not responding to or too young for medication. Further FFD research should focus on establishing the underlying mechanisms of food (e.g. incrimination of gut microbiota) to simplify the FFD approach in children with ADHD.
Conflict of interest statement
LMP is franchiser of the restricted elimination diet (RED) protocol and has received honoraria for applying the RED protocol in the Netherlands. RRP and LMP received travel grants and honoraria for speaking or participations at meetings. RRP is a board member of ADHD in Practice, Impuls & Woortblind and Dutch ADHD Quality Standard. All other authors declare to have no competing interests. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th edn, text revision. Washington, DC: American Psychiatric Association; 2000.
-
- Molina BS, Hinshaw SP, Eugene Arnold L, Swanson JM, Pelham WE, Hechtman L, et al. Adolescent substance use in the multimodal treatment study of attention-deficit/hyperactivity disorder (ADHD) (MTA) as a function of childhood ADHD, random assignment to childhood treatments, and subsequent medication. J Am Acad Child Adolesc Psychiatry. 2013;52(3):250–63. 10.1016/j.jaac.2012.12.014 - DOI - PMC - PubMed
-
- Biederman J, Petty CR, Monuteaux MC, Mick E, Parcell T, Westerberg D, et al. The longitudinal course of comorbid oppositional defiant disorder in girls with attention-deficit/hyperactivity disorder: findings from a controlled 5-year prospective longitudinal follow-up study. J Dev Behav Pediatr. 2008;29(6):501–07. 10.1097/DBP.0b013e318190b290 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
