

Acute high-intensity interval exercise reduces human monocyte Toll-like receptor 2 expression in type 2 diabetes
- PMID: 28122717
- PMCID: PMC5407082
- DOI: 10.1152/ajpregu.00348.2016
Acute high-intensity interval exercise reduces human monocyte Toll-like receptor 2 expression in type 2 diabetes
Abstract
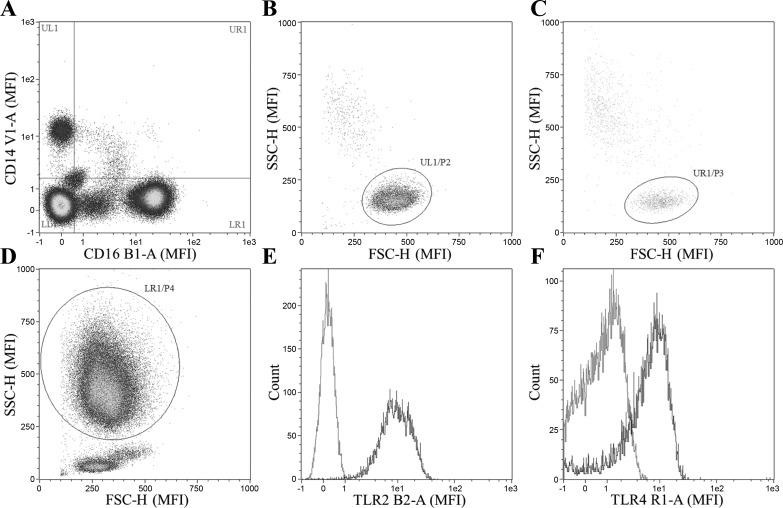
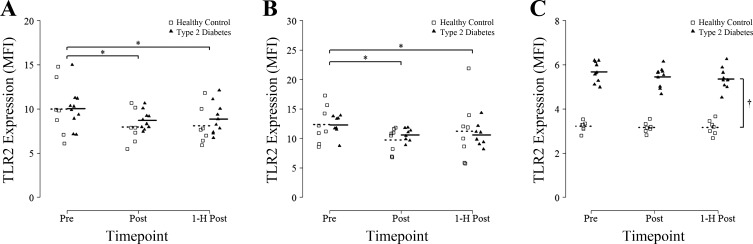
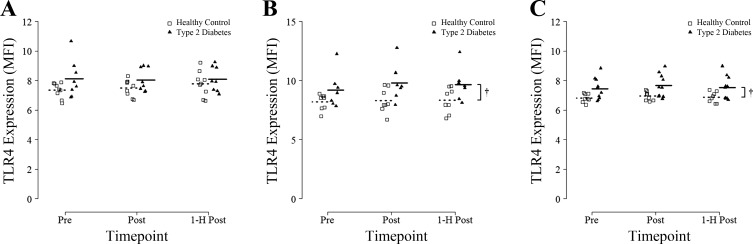
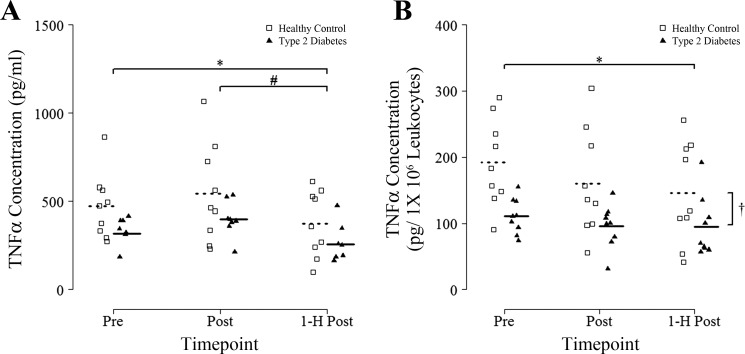
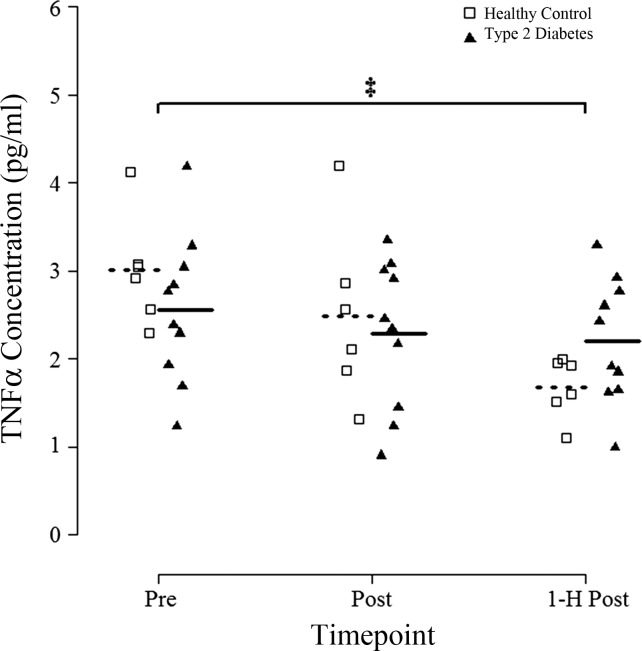
Type 2 diabetes (T2D) is characterized by chronic low-grade inflammation that contributes to disease pathophysiology. Exercise has anti-inflammatory effects, but the impact of high-intensity interval training (HIIT) is not known. The purpose of this study was to determine the impact of a single session of HIIT on cellular, molecular, and circulating markers of inflammation in individuals with T2D. Participants with T2D (n = 10) and healthy age-matched controls (HC; n = 9) completed an acute bout of HIIT (7 × 1 min at ~85% maximal aerobic power output, separated by 1 min of recovery) on a cycle ergometer with blood samples obtained before (Pre), immediately after (Post), and at 1 h of recovery (1-h Post). Inflammatory markers on leukocytes were measured by flow cytometry, and TNF-α was assessed in both LPS-stimulated whole blood cultures and plasma. A single session of HIIT had an overall anti-inflammatory effect, as evidenced by 1) significantly lower levels of Toll-like receptor (TLR) 2 surface protein expression on both classical and CD16+ monocytes assessed at Post and 1-h Post compared with Pre (P < 0.05 for all); 2) significantly lower LPS-stimulated TNF-α release in whole blood cultures at 1-h Post (P < 0.05 vs. Pre); and 3) significantly lower levels of plasma TNF-α at 1-h Post (P < 0.05 vs. Pre). There were no differences between T2D and HC, except for a larger decrease in plasma TNF-α in HC vs. T2D (group × time interaction, P < 0.05). One session of low-volume HIIT has immunomodulatory effects and provides potential anti-inflammatory benefits to people with, and without, T2D.
Keywords: CD14+ monocyte; inflammation; innate immunity; leukocyte; tumor necrosis factor-α.
Copyright © 2017 the American Physiological Society.
Figures
References
-
- American College of Sports Medicine; American Diabetes Association; Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, Chasan-Taber L, Albright AL, Braun B. Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care 33: e147–e167, 2010. doi:10.2337/dc10-9990. - DOI - PMC - PubMed
-
- Balducci S, Zanuso S, Nicolucci A, Fernando F, Cavallo S, Cardelli P, Fallucca S, Alessi E, Letizia C, Jimenez A, Fallucca F, Pugliese G. Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr Metab Cardiovasc Dis 20: 608–617, 2010. doi:10.1016/j.numecd.2009.04.015. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials