

21-Gene Recurrence Score and Locoregional Recurrence in Node-Positive/ER-Positive Breast Cancer Treated With Chemo-Endocrine Therapy
- PMID: 28122895
- PMCID: PMC5721938
- DOI: 10.1093/jnci/djw259
21-Gene Recurrence Score and Locoregional Recurrence in Node-Positive/ER-Positive Breast Cancer Treated With Chemo-Endocrine Therapy
Abstract
Background: The 21-gene recurrence score (RS) predicts risk of locoregional recurrence (LRR) in node-negative, estrogen receptor (ER)-positive breast cancer. We evaluated the association between RS and LRR in node-positive, ER-positive patients treated with adjuvant chemotherapy plus tamoxifen in National Surgical Adjuvant Breast and Bowel Project B-28.
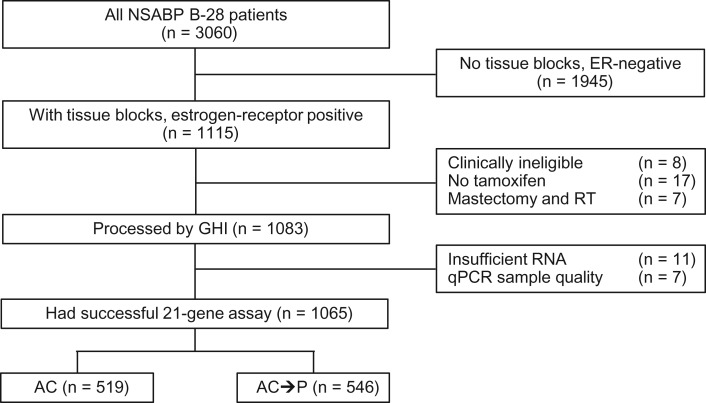
Methods: B-28 compared doxorubicin/cyclophosphamide (AC X 4) with AC X 4 followed by paclitaxel X 4. Tamoxifen was given to patients age 50 years or older and those younger than age 50 years with ER-positive and/or progesterone receptor-positive tumors. Lumpectomy patients received breast radiotherapy. Mastectomy patients received no radiotherapy. The present study includes 1065 ER-positive, tamoxifen-treated patients with RS assessment. Cumulative incidence functions and subdistribution hazard regression models were used for LRR to account for competing risks including distant recurrence, second primary cancers, and death from other causes. Median follow-up was 11.2 years. All statistical tests were one-sided.
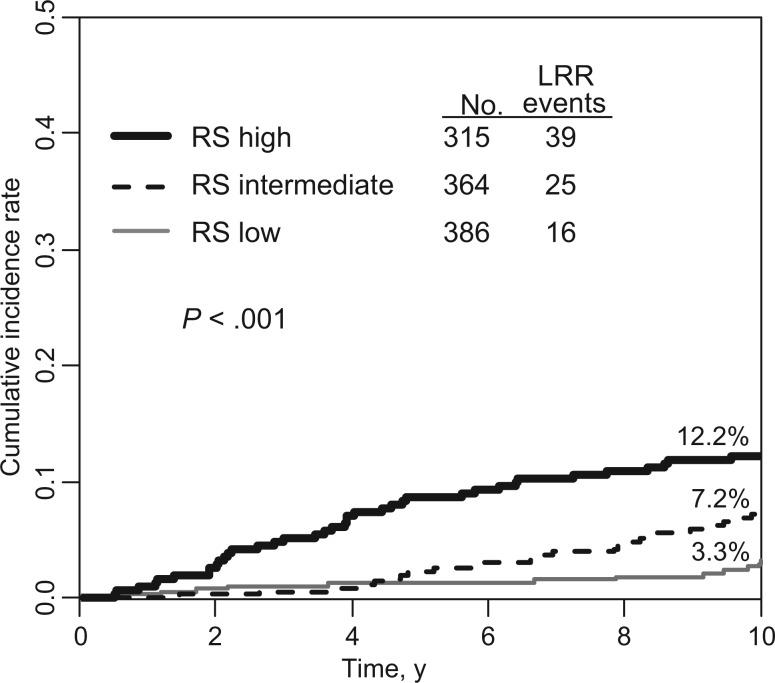
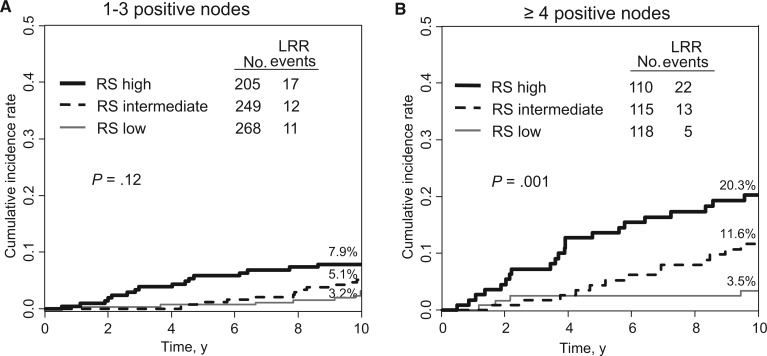
Results: There were 80 LRRs (7.5%) as first events (68% local/32% regional). RS was low: 36.2%; intermediate: 34.2%; and high: 29.6%. RS was a statistically significant predictor of LRR in univariate analyses (10-year cumulative incidence of LRR = 3.3%, 7.2%, and 12.2% for low, intermediate, and high RS, respectively, P < .001). In multivariable regression analysis, RS remained an independent predictor of LRR (hazard ratio [HR] = 2.59, 95% confidence interval [CI] = 1.28 to 5.26, for a 50-point difference, P = .008) along with pathologic nodal status (HR = 1.91, 95% CI = 1.20 to 3.03, for four or more vs one to three positive nodes, P = .006) and tumor size (HR = 1.28, 95% CI = 1.05 to 1.55, for a 1 cm difference, P = .02).
Conclusions: RS statistically significantly predicts risk of LRR in node-positive, ER-positive breast cancer patients after adjuvant chemotherapy plus tamoxifen. These findings can help in the selection of appropriate candidates for comprehensive radiotherapy.
© The Author 2017. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Wapnir IL, Anderson SJ, Mamounas EP, et al. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five National Surgical Adjuvant Breast and Bowel Project node-positive adjuvant breast cancer trials. J Clin Oncol. 2006;2413:2028–2037. - PubMed
-
- Taghian A, Jeong JH, Mamounas E, et al. Patterns of locoregional failure in patients with operable breast cancer treated by mastectomy and adjuvant chemotherapy with or without tamoxifen and without radiotherapy: Results from five National Surgical Adjuvant Breast and Bowel Project randomized clinical trials. J Clin Oncol. 2004;2221:4247–4254. - PubMed
-
- Nguyen PL, Taghian AG, Katz MS, et al. Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. J Clin Oncol. 2008;2618:2373–2378. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
