

Constipation and Incident CKD
- PMID: 28122944
- PMCID: PMC5373459
- DOI: 10.1681/ASN.2016060656
Constipation and Incident CKD
Abstract
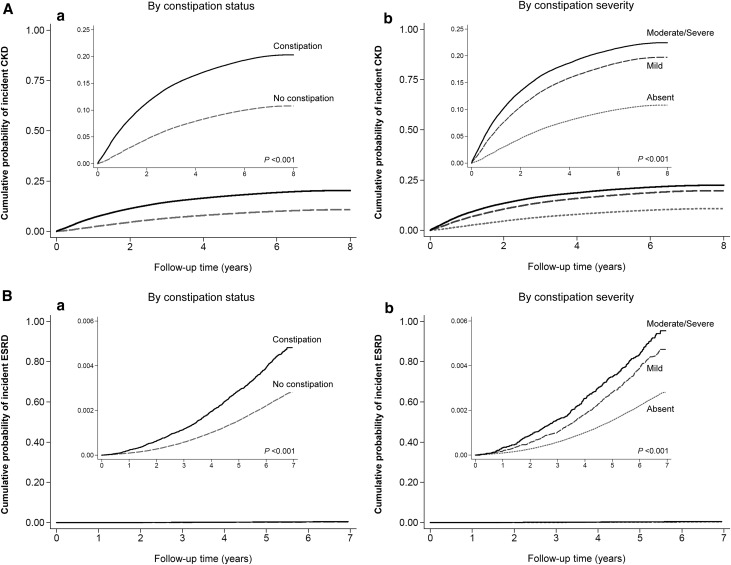
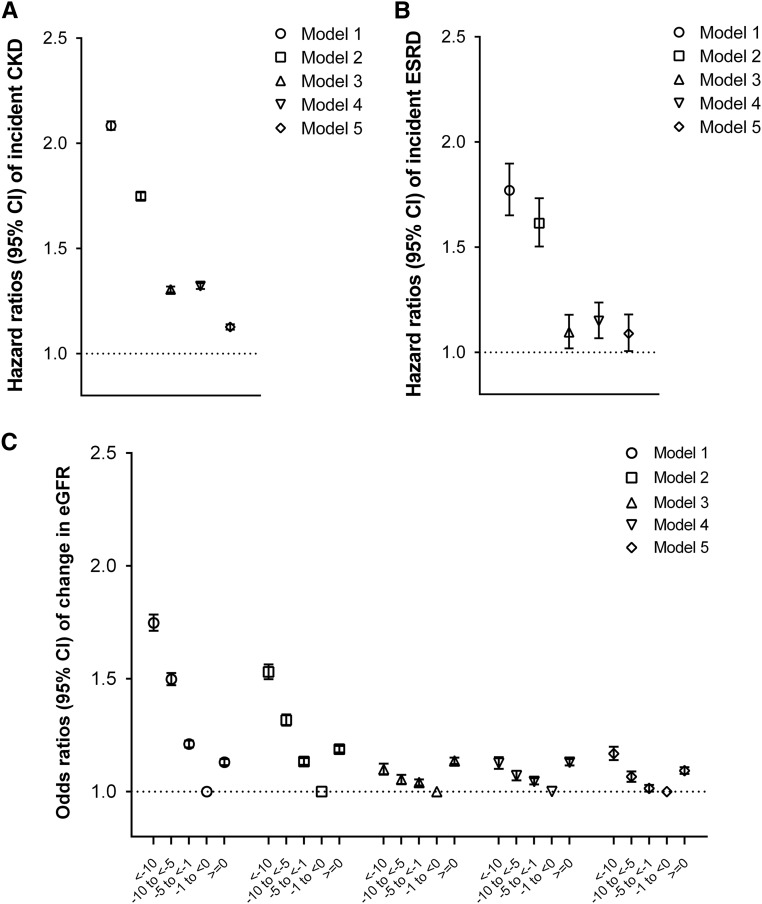
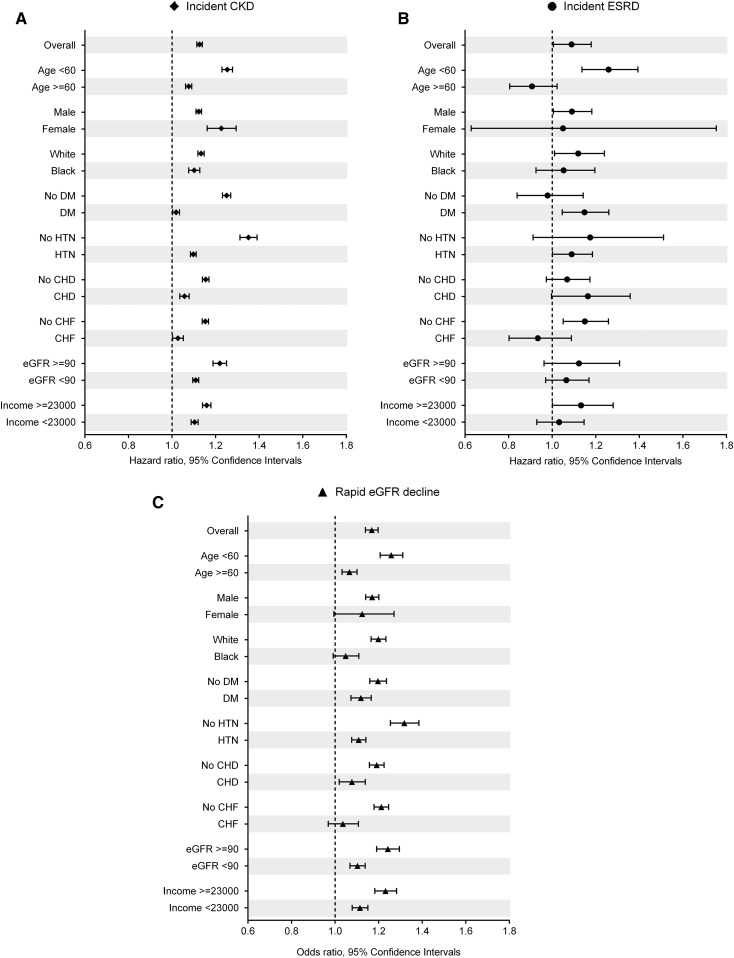
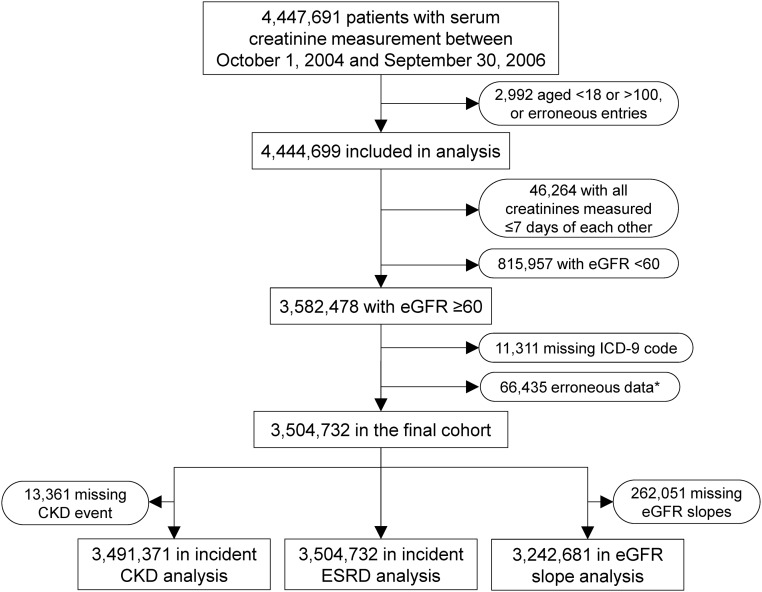
Constipation is one of the most prevalent conditions in primary care settings and increases the risk of cardiovascular disease, potentially through processes mediated by altered gut microbiota. However, little is known about the association of constipation with CKD. In a nationwide cohort of 3,504,732 United States veterans with an eGFR ≥60 ml/min per 1.73 m2, we examined the association of constipation status and severity (absent, mild, or moderate/severe), defined using diagnostic codes and laxative use, with incident CKD, incident ESRD, and change in eGFR in Cox models (for time-to-event analyses) and multinomial logistic regression models (for change in eGFR). Among patients, the mean (SD) age was 60.0 (14.1) years old; 93.2% of patients were men, and 24.7% were diabetic. After multivariable adjustments, compared with patients without constipation, patients with constipation had higher incidence rates of CKD (hazard ratio, 1.13; 95% confidence interval [95% CI], 1.11 to 1.14) and ESRD (hazard ratio, 1.09; 95% CI, 1.01 to 1.18) and faster eGFR decline (multinomial odds ratios for eGFR slope <-10, -10 to <-5, and -5 to <-1 versus -1 to <0 ml/min per 1.73 m2 per year, 1.17; 95% CI, 1.14 to 1.20; 1.07; 95% CI, 1.04 to 1.09; and 1.01; 95% CI, 1.00 to 1.03, respectively). More severe constipation associated with an incrementally higher risk for each renal outcome. In conclusion, constipation status and severity associate with higher risk of incident CKD and ESRD and with progressive eGFR decline, independent of known risk factors. Further studies should elucidate the underlying mechanisms.
Keywords: Epidemiology and outcomes; chronic kidney disease; end-stage renal disease; glomerular filtration rate.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Eckardt KU, Coresh J, Devuyst O, Johnson RJ, Köttgen A, Levey AS, Levin A: Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 382: 158–169, 2013 - PubMed
-
- Levey AS, Coresh J: Chronic kidney disease. Lancet 379: 165–180, 2012 - PubMed
-
- Sun SX, Dibonaventura M, Purayidathil FW, Wagner JS, Dabbous O, Mody R: Impact of chronic constipation on health-related quality of life, work productivity, and healthcare resource use: An analysis of the National Health and Wellness Survey. Dig Dis Sci 56: 2688–2695, 2011 - PubMed
-
- Guerin A, Carson RT, Lewis B, Yin D, Kaminsky M, Wu E: The economic burden of treatment failure amongst patients with irritable bowel syndrome with constipation or chronic constipation: A retrospective analysis of a Medicaid population. J Med Econ 17: 577–586, 2014 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
