

Targeting the MAPK and PI3K pathways in combination with PD1 blockade in melanoma
- PMID: 28123875
- PMCID: PMC5215252
- DOI: 10.1080/2162402X.2016.1238557
Targeting the MAPK and PI3K pathways in combination with PD1 blockade in melanoma
Abstract
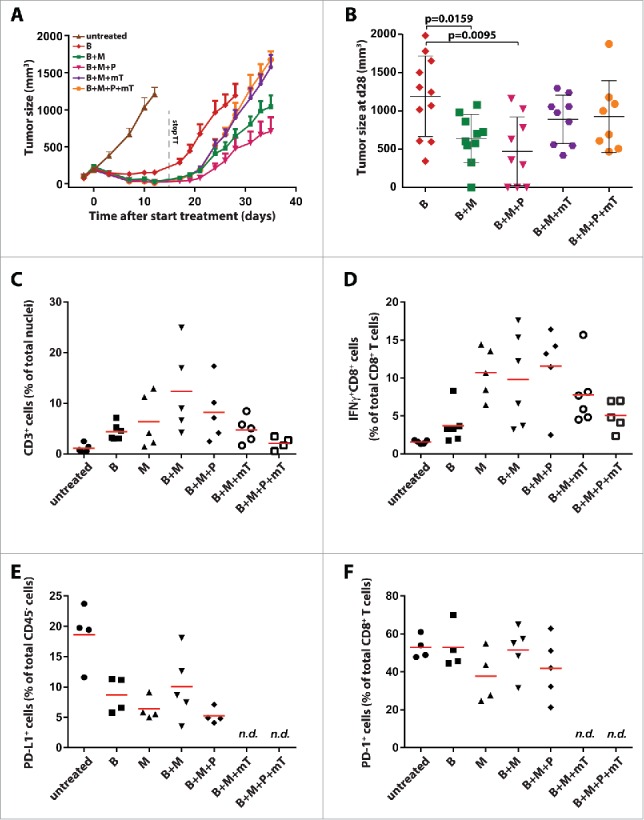
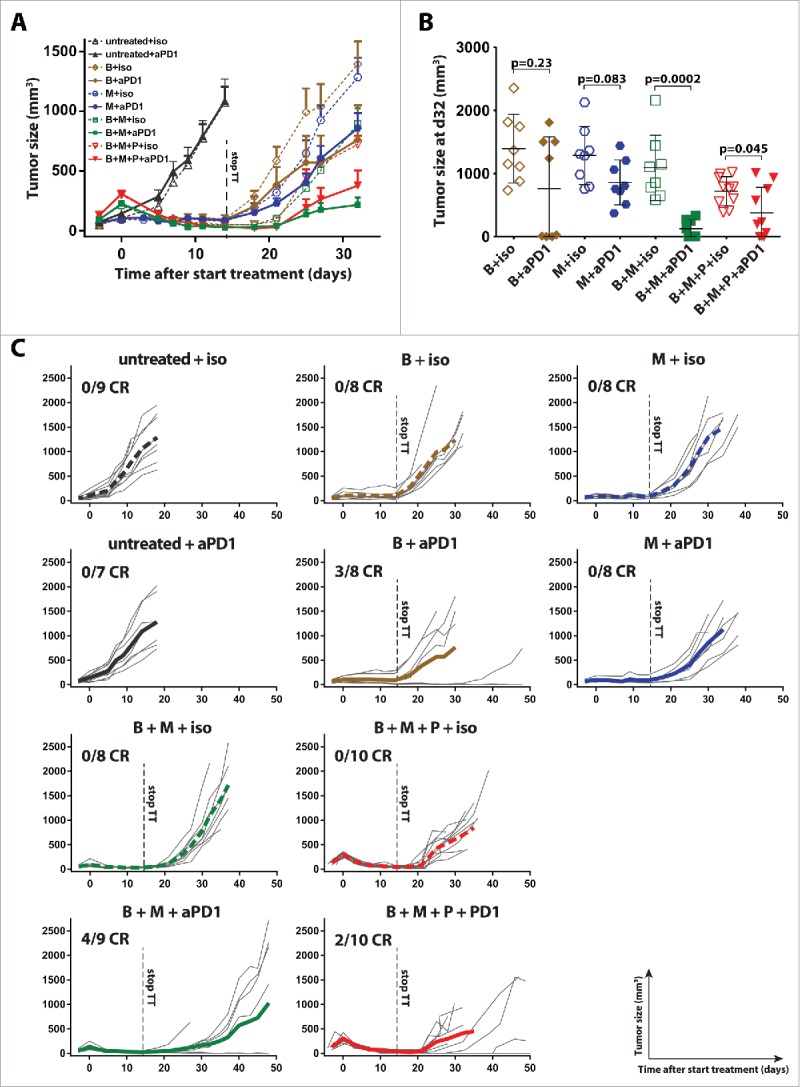
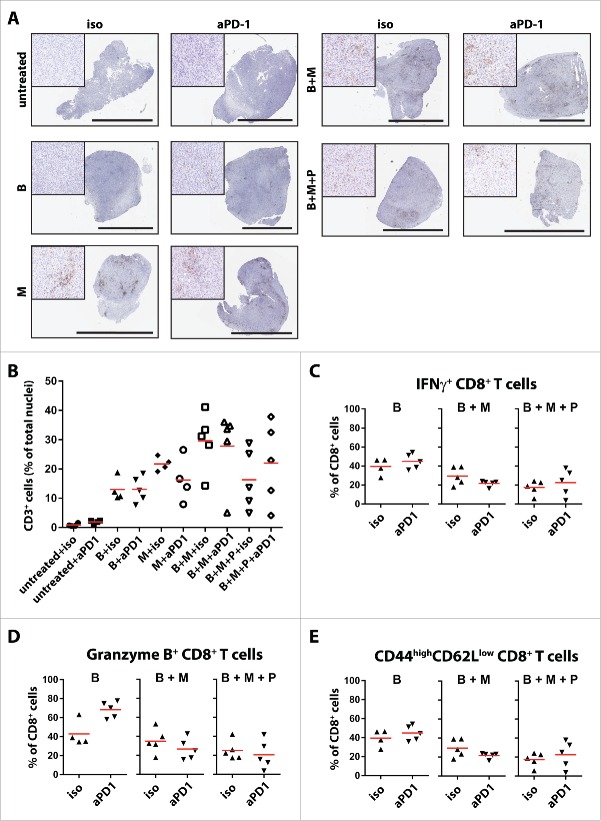
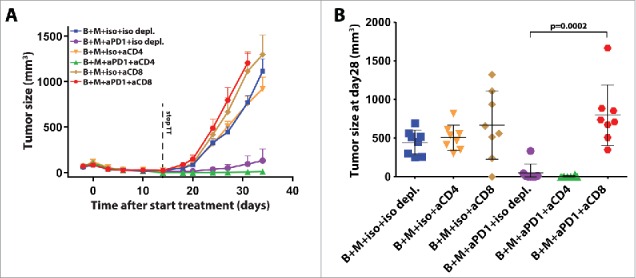
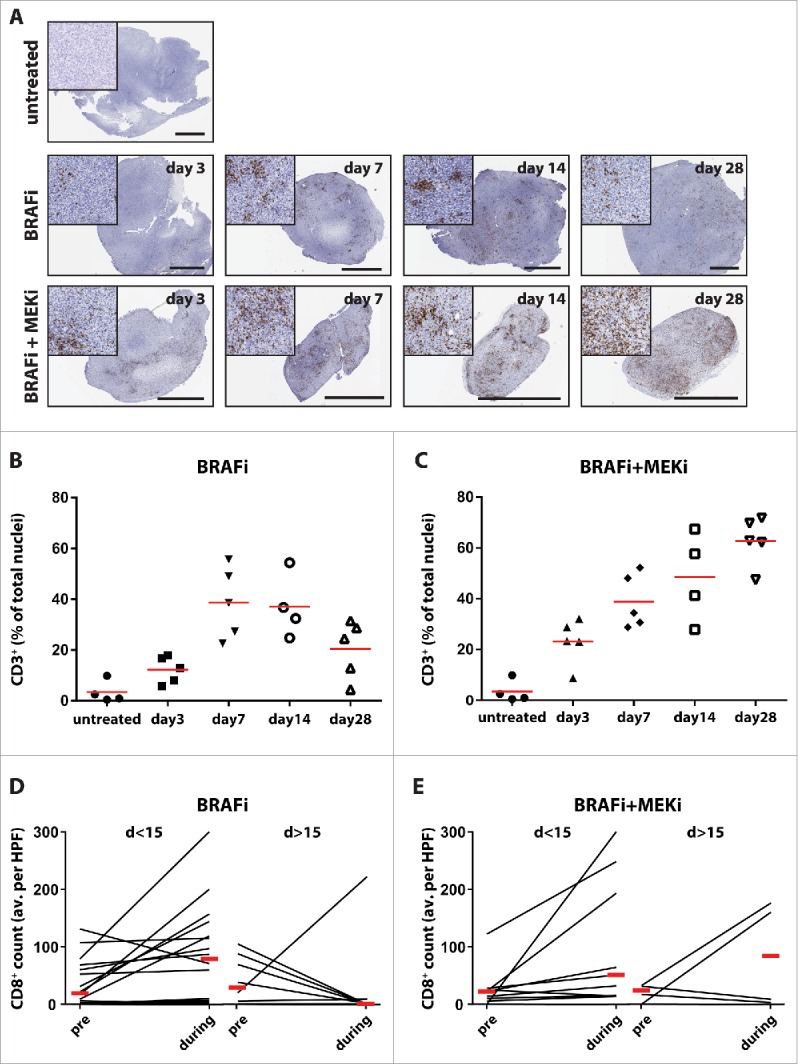
Immunotherapy of advanced melanoma with CTLA-4 or PD-1/PD-L1 checkpoint blockade induces in a proportion of patients long durable responses. In contrast, targeting the MAPK-pathway by selective BRAF and MEK inhibitors induces high response rates, but most patients relapse. Combining targeted therapy with immunotherapy is proposed to improve the long-term outcomes of patients. Preclinical data endorsing this hypothesis are accumulating. Inhibition of the PI3K-Akt-mTOR pathway may be a promising treatment option to overcome resistance to MAPK inhibition and for additional combination with immunotherapy. We therefore evaluated to which extent dual targeting of the MAPK and PI3K-Akt-mTOR pathways affects tumor immune infiltrates and whether it synergizes with PD-1 checkpoint blockade in a BRAFV600E/PTEN-/--driven melanoma mouse model. Short-term dual BRAF + MEK inhibition enhanced tumor immune infiltration and improved tumor control when combined with PD-1 blockade in a CD8+ T cell dependent manner. Additional PI3K inhibition did not impair tumor control or immune cell infiltration and functionality. Analysis of on-treatment samples from melanoma patients treated with BRAF or BRAF + MEK inhibitors indicates that inhibitor-mediated T cell infiltration occurred in all patients early after treatment initiation but was less frequent found in on-treatment biopsies beyond day 15. Our findings provide a rationale for clinical testing of short-term BRAF + MEK inhibition in combination with immune checkpoint blockade, currently implemented at our institutes. Additional PI3K inhibition could be an option for BRAF + MEK inhibitor resistant patients that receive targeted therapy in combination with immune checkpoint blockade.
Keywords: Anti-PD-1; BRAF; MAPK; MEK; PI3K; checkpoint blockade; immunotherapy; mTOR; melanoma; targeted therapy.
Figures
References
-
- Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M et al.. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Eng J Med 2011; 364:2507-16; PMID:21639808; http://dx.doi.org/ 10.1056/NEJMoa1103782 - DOI - PMC - PubMed
-
- Flaherty KT, Robert C, Hersey P, Nathan P, Garbe C, Milhem M, Demidov LV, Hassel JC, Rutkowski P, Mohr P et al.. Improved survival with MEK inhibition in BRAF-mutated melanoma. N Eng J Med 2012; 367:107-14; PMID:22663011; http://dx.doi.org/ 10.1056/NEJMoa1203421 - DOI - PubMed
-
- Mizugaki H, Yamamoto N, Murakami H, Kenmotsu H, Fujiwara Y, Ishida Y, Kawakami T, Takahashi T et al.. Phase I dose-finding study of monotherapy with atezolizumab, an engineered immunoglobulin monoclonal antibody targeting PD-L1, in Japanese patients with advanced solid tumors. Invest New Drugs 2016; 34(5):596-603; PMID:27363843; http://dx.doi.org/ 10.1007/s10637-016-0371-6 - DOI - PMC - PubMed
-
- Ribas A, Puzanov I, Dummer R, Schadendorf D, Hamid O, Robert C, Hodi FS, Schachter J, Pavlick AC, Lewis KD et al.. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. The Lancet Oncol 2015; 16:908-18; PMID:26115796; http://dx.doi.org/ 10.1016/S1470-2045(15)00083-2 - DOI - PMC - PubMed
-
- Robert C, Long GV, Brady B, Dutriaux C, Maio M, Mortier L, Hassel JC, Rutkowski P, McNeil C, Kalinka-Warzocha E et al.. Nivolumab in previously untreated melanoma without BRAF mutation. N Eng J Med 2015; 372:320-30; PMID:25399552; http://dx.doi.org/ 10.1056/NEJMoa1412082 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous