

Epidemiology of Pediatric Critical Illness in a Population-Based Birth Cohort in Olmsted County, MN
- PMID: 28125547
- PMCID: PMC5336468
- DOI: 10.1097/PCC.0000000000001084
Epidemiology of Pediatric Critical Illness in a Population-Based Birth Cohort in Olmsted County, MN
Abstract
Objectives: Investigations of pediatric critical illness typically focus on inpatient cohorts drawn from wide referral areas and diverse healthcare systems. Cohorts amenable to investigating the full spectrum of critical illness as it develops within a community have yet to be studied in the United States. Our objective was to provide the first epidemiologic report of the incidence and presentation of pediatric critical illness within a U.S. population-based birth cohort.
Design: Retrospective cohort study.
Setting: A geographically defined community (Olmsted, MN) with medical record linkage across all health systems. All ICU services are provided within a single children's hospital.
Patients: A birth cohort of children (n =9,441) born 2003-2007 in Olmsted County, MN.
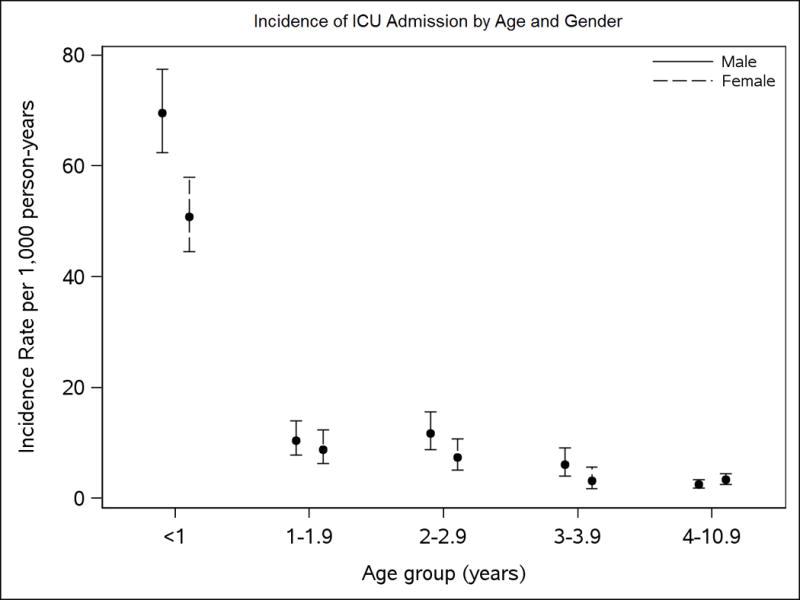
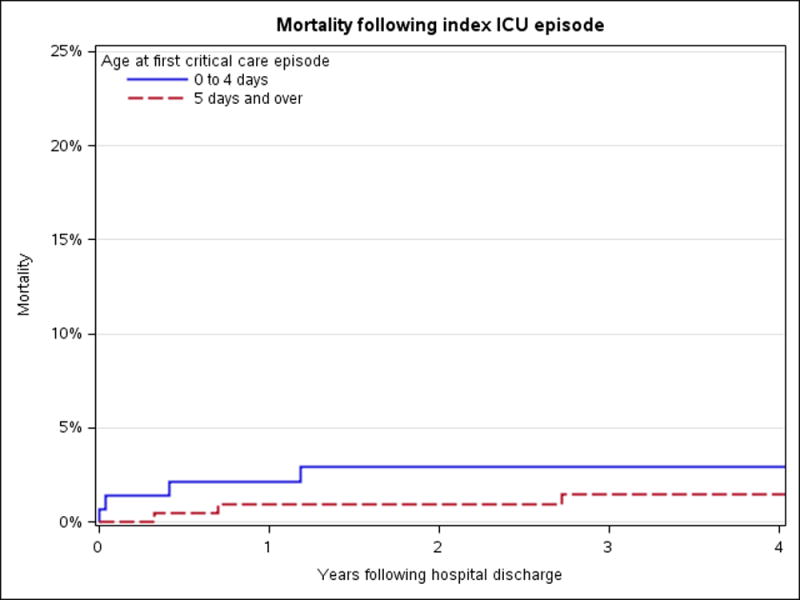
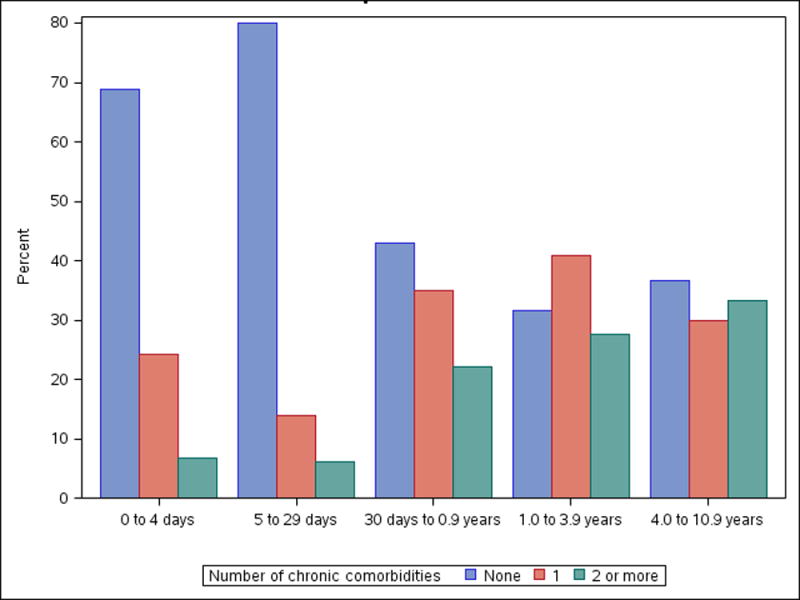
Measurements and main results: During the study period, there were a total of 15,277 ICU admissions to Mayo Clinic Children's Hospital. A total of 577 birth cohort children accounted for 824 of these admissions during the 61,770 person-years of follow-up accumulated. Incidence of first-time ICU admission was 9.3 admits per 1,000 person-years. Admission rates were highest in the first year of life and then declined steadily. Respiratory problems were among the most common reasons for admission at any age and diagnoses reflect changes in health risk factors as children grow and develop over time. After 1 year old, a majority of children admitted have preexisting chronic comorbidities and/or prior ICU stays. In-hospital mortality occurred exclusively in children admitted prior to 5 days of age (n = 4). Seven children died after hospital discharge.
Conclusions: This is the first report characterizing critical illness within a population-based birth cohort of U.S. children. The results demonstrate the changing incidence, presentation, and healthcare requirements associated with critical illness across the developmental spectrum as a population of children ages.
Figures
References
-
- Namachivayam P, Shann F, Shekerdemian L, et al. Three decades of pediatric intensive care: Who was admitted, what happened in intensive care, and what happened afterward. Pediatr Crit Care Med. 2010;11:549–555. - PubMed
-
- Aspesberro F, Mangione-Smith R, Zimmerman JJ. Health-related quality of life following pediatric critical illness. Intensive Care Med. 2015;41:1235–1246. - PubMed
-
- Nicholson CE, Gans BM, Chang AC, et al. Pediatric critical care medicine: Planning for our research future. Pediatr Crit Care Med. 2003;4:196–202. - PubMed
-
- Williams TA, Dobb GJ, Finn JC, et al. Determinants of long-term survival after intensive care. Crit Care Med. 2008;36:1523–1530. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
