

Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing
- PMID: 28125772
- PMCID: PMC6464914
- DOI: 10.1002/14651858.CD005122.pub5
Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing
Abstract
Background: The admission cardiotocograph (CTG) is a commonly used screening test consisting of a short (usually 20 minutes) recording of the fetal heart rate (FHR) and uterine activity performed on the mother's admission to the labour ward. This is an update of a review published in 2012.
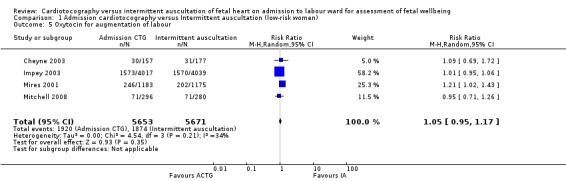
Objectives: To compare the effects of admission cardiotocography with intermittent auscultation of the FHR on maternal and infant outcomes for pregnant women without risk factors on their admission to the labour ward.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register to 30 November 2016 and we planned to review the reference list of retrieved papers
Selection criteria: All randomised and quasi-randomised trials comparing admission CTG with intermittent auscultation of the FHR for pregnant women between 37 and 42 completed weeks of pregnancy and considered to be at low risk of intrapartum fetal hypoxia and of developing complications during labour.
Data collection and analysis: Two authors independently assessed trial eligibility and quality, and extracted data. Data were checked for accuracy.
Main results: We included no new trials in this update. We included four trials involving more than 13,000 women which were conducted in the UK and Ireland and included women in labour. Three trials were funded by the hospitals where the trials took place and one trial was funded by the Scottish government. No declarations of interest were made in two trials; the remaining two trials did not mention declarations of interest. Overall, the studies were assessed as low risk of bias. Results reported in the 2012 review remain unchanged.Although not statistically significant using a strict P < 0.05 criterion, data were consistent with women allocated to admission CTG having, on average, a higher probability of an increase in incidence of caesarean section than women allocated to intermittent auscultation (risk ratio (RR) 1.20, 95% confidence interval (CI) 1.00 to 1.44, 4 trials, 11,338 women, I² = 0%, moderate quality evidence). There was no clear difference in the average treatment effect across included trials between women allocated to admission CTG and women allocated to intermittent auscultation in instrumental vaginal birth (RR 1.10, 95% CI 0.95 to 1.27, 4 trials, 11,338 women, I² = 38%, low quality evidence) and perinatal mortality rate (RR 1.01, 95% CI 0.30 to 3.47, 4 trials, 11,339 infants, I² = 0%, moderate quality evidence).Women allocated to admission CTG had, on average, higher rates of continuous electronic fetal monitoring during labour (RR 1.30, 95% CI 1.14 to 1.48, 3 trials, 10,753 women, I² = 79%, low quality evidence) and fetal blood sampling (RR 1.28, 95% CI 1.13 to 1.45, 3 trials, 10,757 women, I² = 0%) than women allocated to intermittent auscultation. There were no differences between groups in other secondary outcome measures including incidence and severity of hypoxic ischaemic encephalopathy (incidence only reported) (RR 1.19, 95% CI 0.37 to 3.90; 2367 infants; 1 trial; very low quality evidence) and incidence of seizures in the neonatal period (RR 0.72, 95% CI 0.32 to 1.61; 8056 infants; 1 trial; low quality evidence). There were no data reported for severe neurodevelopmental disability assessed at greater than, or equal to, 12 months of age.
Authors' conclusions: Contrary to continued use in some clinical areas, we found no evidence of benefit for the use of the admission CTG for low-risk women on admission in labour.Furthermore, the probability is that admission CTG increases the caesarean section rate by approximately 20%. The data lacked power to detect possible important differences in perinatal mortality. However, it is unlikely that any trial, or meta-analysis, will be adequately powered to detect such differences. The findings of this review support recommendations that the admission CTG not be used for women who are low risk on admission in labour. Women should be informed that admission CTG is likely associated with an increase in the incidence of caesarean section without evidence of benefit.Evidence quality ranged from moderate to very low, with downgrading decisions based on imprecision, inconsistency and a lack of blinding for participants and personnel. All four included trials were conducted in developed Western European countries. One additional study is ongoing.The usefulness of the findings of this review for developing countries will depend on FHR monitoring practices. However, an absence of benefit and likely harm associated with admission CTG will have relevance for countries where questions are being asked about the role of the admission CTG.Future studies evaluating the effects of the admission CTG should consider including women admitted with signs of labour and before a formal diagnosis of labour. This would include a cohort of women currently having admission CTGs and not included in current trials.
Conflict of interest statement
Declan Devane is currently conducting a trial, known as the ADCAR Trial, evaluating the effectiveness of the admission cardiotocograph (CTG) compared with intermittent auscultation. This study is funded by the Health Research Board (Ireland). If this trial is eligible for inclusion in the full review, or a subsequent review update, the investigators will not be involved in assessing the trial for inclusion, assessing risk of bias, or data extraction. These tasks will be carried out by two other members of the review team who are not directly involved with the ADCAR Trial.
Joan G Lalor: none known.
Sean Daly: none known.
William McGuire: none known.
Anna Cuthbert: none known.
Valerie Smith: is currently conducting a trial, known as the ADCAR Trial, evaluating the effectiveness of the admission cardiotocograph (CTG) compared with intermittent auscultation. This study is funded by the Health Research Board (Ireland). If this trial is eligible for inclusion in the full review, or a subsequent review update, the investigators will not be involved in assessing the trial for inclusion, assessing risk of bias, or data extraction. These tasks will be carried out by two other members of the review team who are not directly involved with the ADCAR Trial.
Figures
















Update of
-
Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing.Cochrane Database Syst Rev. 2012 Feb 15;(2):CD005122. doi: 10.1002/14651858.CD005122.pub4. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2017 Jan 26;1:CD005122. doi: 10.1002/14651858.CD005122.pub5. PMID: 22336808 Updated.
Comment in
-
Cardiotocography versus intermittent auscultation of foetal heart on admission to labour ward for assessment of foetal wellbeing.Int J Nurs Pract. 2018 Jun;24(3):e12613. doi: 10.1111/ijn.12613. Epub 2017 Nov 21. Int J Nurs Pract. 2018. PMID: 29159882 No abstract available.
-
Cardiotocography vs. Intermittent Auscultation in Assessing Fetal Well-Being.Am J Nurs. 2018 Jun;118(6):23. doi: 10.1097/01.NAJ.0000534845.27761.cc. Am J Nurs. 2018. PMID: 29794915
References
References to studies included in this review
Cheyne 2003 {published data only}
-
- Cheyne H, Dunlop A, Shields N, Mathers AM. A randomised controlled trial of admission electronic fetal monitoring in normal labour. Midwifery 2003;19(3):221‐9. - PubMed
Impey 2003 {published data only}
-
- Impey L, Reynolds M, MacQuillan K, Gates S, Murphy J, Sheil O. Admission cardiotocography: a randomised controlled trial. Lancet 2003;361(9356):465‐70. - PubMed
Mires 2001 {published data only}
Mitchell 2008 {published data only}
-
- ISRCTN28370122. A randomised controlled trial evaluating the relationship between the labour electronic fetal monitoring (EFM) admission test and obstetric intervention in low risk mothers. isrctn.com/ISRCTN28370122 Date first received: 12 September 2003.
-
- Mitchell K. The effect of the labour electronic fetal monitoring admission test on operative delivery in low‐risk women: a randomised controlled trial. Evidence Based Midwifery 2008;6(1):18‐26.
References to ongoing studies
Devane 2008 {published data only}
-
- ISRCTN96340041. A randomised controlled trial comparing the effect of admission cardiotocography versus intermittent auscultation of the foetal heart rate on low‐risk women on admission to labour ward showing signs of possible labour. isrctn.com/ISRCTN96340041 Date first received: 25 March 2008.
Additional references
Alfirevic 2013
Arulkumaran 2000
-
- Arulkumaran S, Jenkins HML. Perinatal Asphyxia. Chennai: Orient Longman Ltd, 2000.
Ayres‐de‐Campos 2015
-
- Ayres‐de‐Campos D, Spong CY, Chandraharan E. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. International Journal of Gynaecology and Obstetrics 2015;131(1):13‐24. - PubMed
Bayley 1993
-
- Bayley N. Manual for the Bayley Scales of Infant Development. 2nd Edition. San Antonio: The Psychological Corporation, 1993.
Brown 2008
Caldeyro‐Barcia 1966
-
- Caldeyro‐Barcia R, Mendez‐Bauer C, Poseiro JJ, Escarcena LA, Pose SV, Bieniarz J, et al. Control of human fetal heart rate during labour. In: Cassels DE editor(s). The Heart and Circulation in the Newborn and Infant. New York: Grune and Stratton, 1966:7‐36.
CESDI 2001
-
- Maternal and Child Health Research Consortium. Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI): 8th Annual Report. London: Maternal and Child Health Research Consortium, 2001.
Devane 2007
-
- Devane D, Lalor J, Bonnar J. The use of intrapartum electronic fetal heart rate monitoring: a national survey. Irish Medical Journal 2007;100(2):360‐2. [PUBMED: 17432809] - PubMed
East 2013
-
- East CE, Smyth RMD, Leader LR, Henshall NE, Colditz PB, Lau R, et al. Vibroacoustic stimulation for fetal assessment in labour in the presence of a nonreassuring fetal heart rate trace. Cochrane Database of Systematic Reviews 2013, Issue 1. [DOI: 10.1002/14651858.CD004664] - DOI
Gail‐Thomas 2003
-
- Gail‐Thomas B. The disempowering concept of risk. In: Wickham S editor(s). Midwifery Best Practice. London: Books for Midwives Press, 2003:3‐6.
Gourounti 2007
-
- Gourounti K, Sandall J. Admission cardiotocography versus intermittent auscultation of fetal heart rate: effects on neonatal Apgar score, on the rate of Caesarean sections and on the rate of instrumental delivery. A systematic review. International Journal of Nursing Studies 2007;44(6):1029‐1035. - PubMed
Grivell 2012
Grivell 2015
Hammacher 1968
-
- Hammacher K, Hūter K, Bokelmann J, Werners P. Foetal heart frequency and perinatal condition of the foetus and newborn. Gynecologica 1968;166(4):349‐60. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Holzmann 2010
-
- Holzmann M, Nordström L. Follow‐up national survey (Sweden) of routines for intrapartum fetal surveillance. Acta Obstetricia et Gynecologica Scandinavica 2010;89(5):712‐4. - PubMed
Hon 1958
-
- Hon EH. The electronic evaluation of the fetal heart rate; preliminary report. American Journal of Obstetrics and Gynecology 1958;75(6):1215‐30. - PubMed
Kaczorowski 1998
-
- Kaczorowski J, Levitt C, Hanvey L, Avard D, Chance G. A national survey of use of obstetric procedures and technologies in Canadian hospitals: routine or based on existing evidence?. Birth 1998;25(1):11‐8. - PubMed
Lalor 2008
Liston 2007
-
- Liston R, Sawchuck D, Young D, Society of Obstetrics and Gynaecologists of Canada, British Columbia Perinatal Health Program. Fetal health surveillance: antepartum and intrapartum consensus guideline. Journal of Obstetrics and Gynaecology Canada 2007;29(9 Suppl 4):S3‐56. - PubMed
MacLennan 1999
Mangesi 2015
Nabhan 2008
NCCWCH 2007
-
- National Collaborating Centre for Women’s and Children’s Health. Intrapartum Care: Care of Healthy Women and Their Babies During Childbirth. London: RCOG Press, 2007. - PubMed
Neilson 2012
Nelson 1996
-
- Nelson KB, Dambrosia JM, Ting TY, Grether JK. Uncertain value of electronic fetal monitoring in predicting cerebral palsy. New England Journal of Medicine 1996;334(10):613‐8. - PubMed
RANZCOG 2002
-
- Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Clinical Guidelines: Intrapartum Surveillance. East Melbourne: RANZCOG, 2002.
RCOG 2001
-
- Royal College of Obstetricians and Gynaecologists. The Use of Electronic Fetal Monitoring: the Use and Interpretation of Cardiotocography in Intrapartum Fetal Surveillance. Evidence‐based Clinical Guideline Number 8. London: Royal College of Obstetricians and Gynaecologists, 2001.
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sarnat 1976
-
- Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress: a clinical and electrographic study. Archives of Neurology 1976;33(10):696‐705. - PubMed
Stampalija 2010
Tan 2012
Tan 2013a
Tan 2013b
WHO 1999
-
- World Health Organization. Care in Normal Birth: a Practical Guide. Report of a Technical Working Group. Geneva: World Health Organization, 1999.
References to other published versions of this review
Devane 2010
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources