

The predictive and prognostic value of tumour necrosis in muscle invasive bladder cancer patients receiving radiotherapy with or without chemotherapy in the BC2001 trial (CRUK/01/004)
- PMID: 28125821
- PMCID: PMC5344298
- DOI: 10.1038/bjc.2017.2
The predictive and prognostic value of tumour necrosis in muscle invasive bladder cancer patients receiving radiotherapy with or without chemotherapy in the BC2001 trial (CRUK/01/004)
Abstract
Background: Severe chronic hypoxia is associated with tumour necrosis. In patients with muscle invasive bladder cancer (MIBC), necrosis is prognostic for survival following surgery or radiotherapy and predicts benefit from hypoxia modification of radiotherapy. Adding mitomycin C (MMC) and 5-fluorouracil (5-FU) chemotherapy to radiotherapy improved locoregional control (LRC) compared to radiotherapy alone in the BC2001 trial. We hypothesised that tumour necrosis would not predict benefit for the addition of MMC and 5-FU to radiotherapy, but would be prognostic.
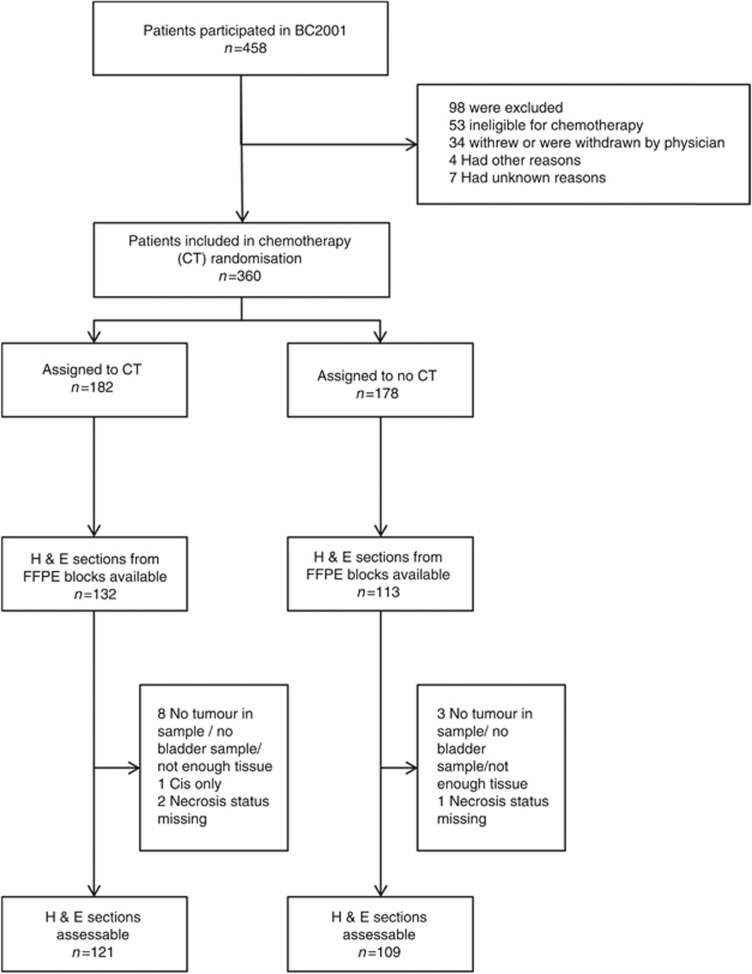
Methods: Diagnostic tumour samples were available from 230 BC2001 patients. Tumour necrosis was scored on whole-tissue sections as absent or present, and its predictive and prognostic significance explored using Cox proportional hazards models. Survival estimates were obtained by Kaplan-Meier methods.
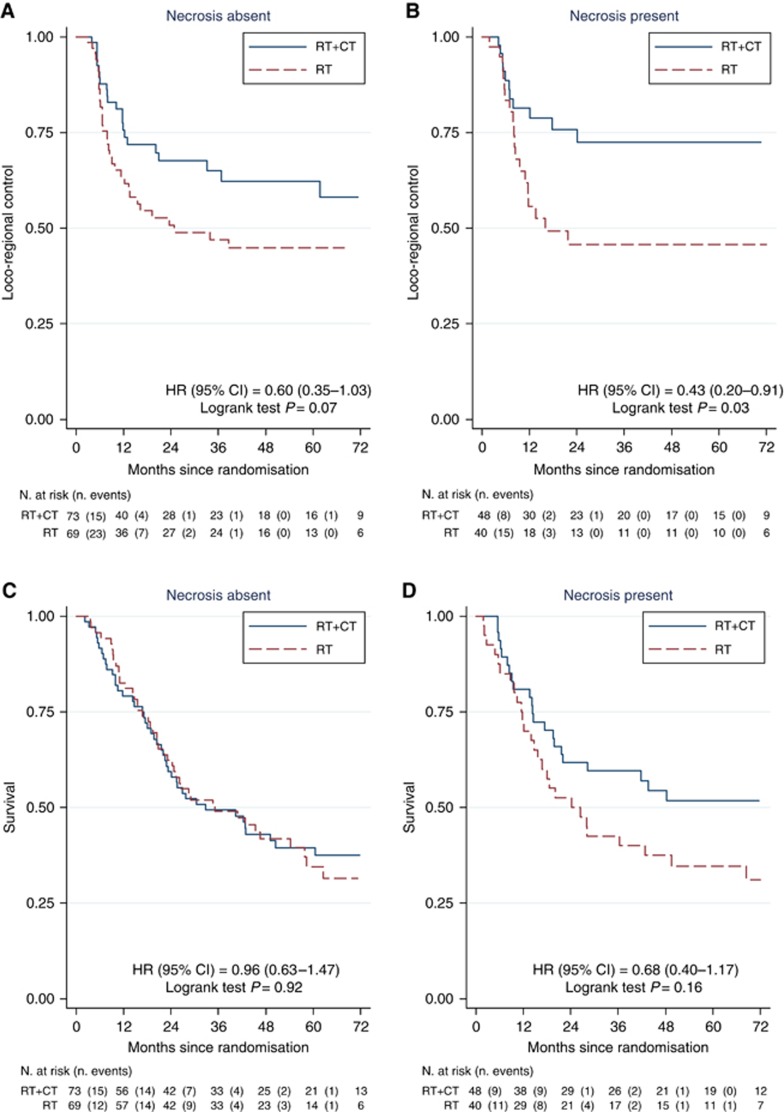
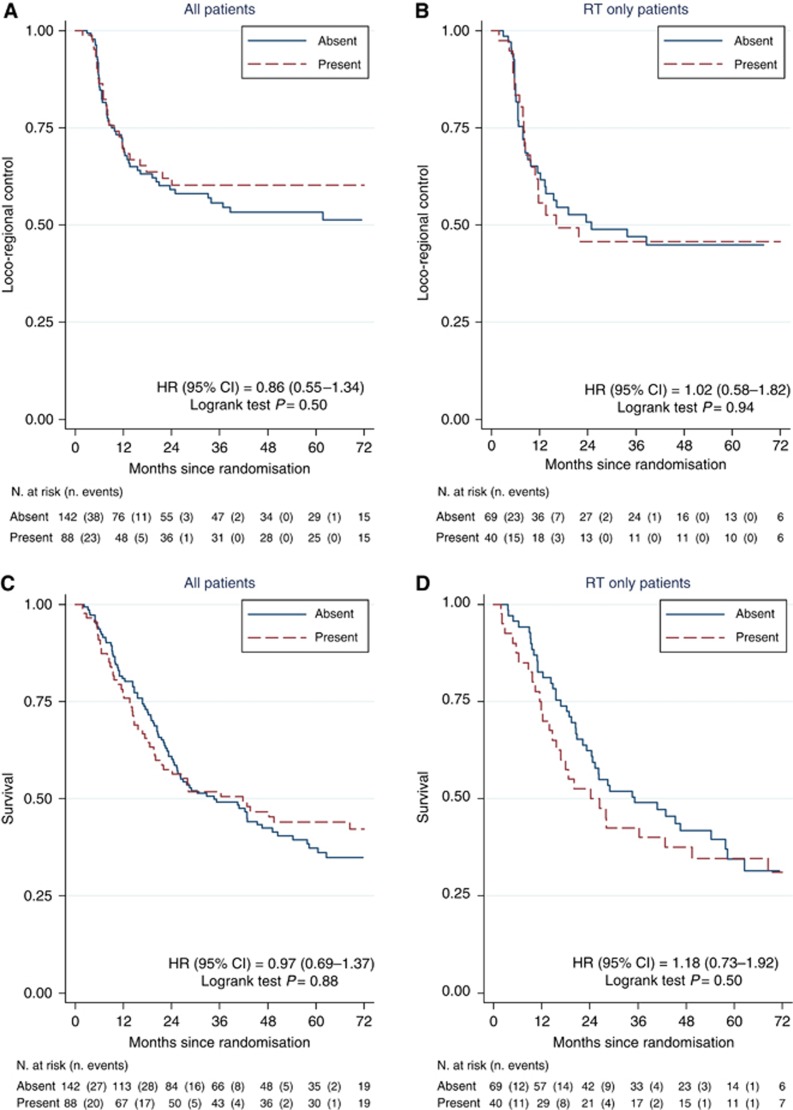
Results: Tumour necrosis was present in 88/230 (38%) samples. Two-year LRC estimates were 71% (95% CI 61-79%) for the MMC/5-FU chemoradiotherapy group and 49% (95% CI 38-59%) for the radiotherapy alone group. When analysed by tumour necrosis status, the adjusted hazard ratios (HR) for MMC/5-FU vs. no chemotherapy were 0.46 (95% CI: 0.12-0.99; P=0.05, necrosis present) and 0.55 (95% CI: 0.31-0.98; P=0.04, necrosis absent). Multivariable analysis of prognosis for LRC by the presence vs. absence of necrosis yielded a HR=0.89 (95% CI 0.55-1.44, P=0.65). There was no significant association for necrosis as a predictive or prognostic factor with respect to overall survival.
Conclusions: Tumour necrosis was neither predictive nor prognostic, and therefore MMC/5-FU is an appropriate radiotherapy-sensitising treatment in MIBC independent of necrosis status.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Booth CM, Siemens DR, Li G, Peng Y, Kong W, Berman DM, Mackillop WJ (2014) Curative therapy for bladder cancer in routine clinical practice: a population-based outcomes study. Clin Oncol (R Coll Radiol) 26: 506–514. - PubMed
-
- Choudhury A, Swindell R, Logue JP, Elliott PA, Livsey JE, Wise M, Symonds P, Wylie JP, Ramani V, Sangar V, Lyons J, Bottomley I, McCaul D, Clarke NW, Kiltie AE, Cowan RA (2011) Phase II study of conformal hypofractionated radiotherapy with concurrent gemcitabine in muscle-invasive bladder cancer. J Clin Oncol 29: 733–738. - PubMed
-
- Eustace A, Irlam JJ, Taylor J, Denley H, Agrawal S, Choudhury A, Ryder D, Ord JJ, Harris AL, Rojas AM, Hoskin PJ, West CM (2013) Necrosis predicts benefit from hypoxia-modifying therapy in patients with high risk bladder cancer enrolled in a phase III randomised trial. Radiother Oncol 108: 40–47. - PMC - PubMed
-
- Hoskin PJ, Rojas AM, Bentzen SM, Saunders MI (2010) Radiotherapy with concurrent carbogen and nicotinamide in bladder carcinoma. J Clin Oncol 28: 4912–4918. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
