

I-Gel is a suitable alternative to endotracheal tubes in the laparoscopic pneumoperitoneum and trendelenburg position
- PMID: 28125979
- PMCID: PMC5267400
- DOI: 10.1186/s12871-016-0291-1
I-Gel is a suitable alternative to endotracheal tubes in the laparoscopic pneumoperitoneum and trendelenburg position
Abstract
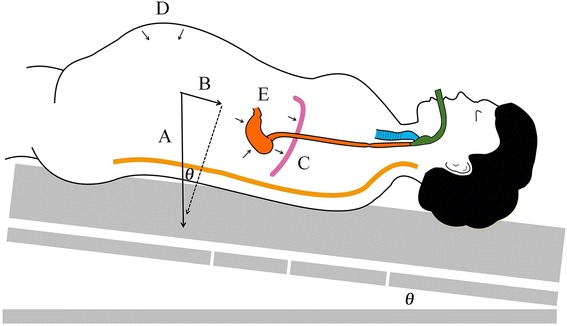
Background: The use of supraglottic airway devices (SADs) in surgeries with laparoscopic pneumoperitoneum and Trendelenburg (LPT) positioning is controversial due to concerns about insufficient pulmonary ventilation and aspiration. In this prospective, randomized-controlled trial, we evaluated whether the i-gel, a new second generation SAD, provides an effective alternative to an endotracheal tube (ETT) by comparing respiratory parameters and perioperative respiratory complications in non-obese patients.
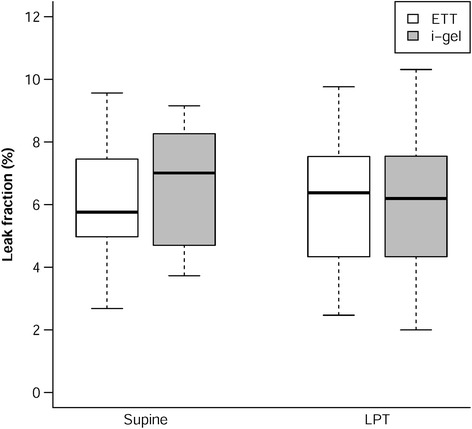
Methods: In a randomized controlled trial, forty anesthetized patients with ASA I-II were divided into equally sized i-gel and ETT groups. We evaluated the respiratory parameters in the supine and LPT position in comparison between the two groups. The leak fraction was our primary outcome, which was defined as the leak volume divided by the inspired tidal volume. The leak volume was the difference between the inspired and expired tidal volumes. We also monitored pulmonary aspiration and respiratory complications during the perioperative period.
Results: In the LPT position, there were no differences in the leak fraction (median [IQR]) between the i-gel and ETT groups (6.20[3.49] vs 6.38[3.71] %, P = 0.883). In the i-gel group, notably less leakage was observed in the LPT position than in the supine position (median [IQR]: 7.01[3.73] %). This phenomenon was not observed in the ETT group. The rate of postoperative sore throat was also significantly lower in the i-gel group than in the ETT group (3/17 vs 9/11). No vomitus nor any signs associated with aspiration were noted in our patients after extubation in the follow-up prior to discharge.
Conclusions: The i-gel provides a suitable alternative to an ETT for surgeries with LPT positioning in non-obese patients.
Trial registration: Registered at Clinicaltrials.gov NCT02462915 , registered on 1 June 2015.
Keywords: Endotracheal tube; Laparoscopic surgery; Leak fraction; Pneumoperitoneum; Respiratory parameters; Trendelenburg position; i-gel.
Figures


References
-
- Ng A, Smith G. Gastroesophageal reflux and aspiration of gastric contents in anesthetic practice. Anesth Analg. 2001;93:494–513. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
