

Barriers to accessing urethroplasty
- PMID: 28127260
- PMCID: PMC5260948
- DOI: 10.3909/riu0731
Barriers to accessing urethroplasty
Abstract
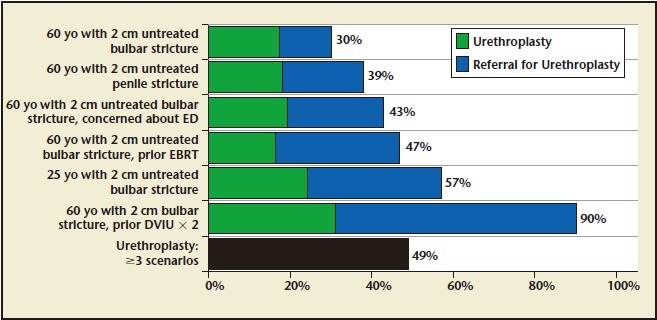
Urethroplasty is an effective treatment for men with anterior urethral strictures, but is utilized less frequently than ineffective treatments such as internal urethrotomy. We sought to identify provider-level barriers to urethroplasty. An anonymous online survey was emailed to all Mid-Atlantic American Urological Association members. Six scenarios in which urethroplasty was the most appropriate treatment were presented. Primary outcome was recommendation for urethroplasty in ≥ three clinical scenarios. Other factors measured include practice zip code, urethroplasty training, and proximity to a urethroplasty surgeon. Multivariate logistic regression identified factors associated with increased likelihood of urethroplasty recommendation. Of 670 members emailed, 109 (16%) completed the survey. Final analysis included 88 respondents. Mean years in practice was 17.2. Most respondents received formal training in urethroplasty: 43 (49%) in residency, 5 (6%) in fellowship, and 10 (11%) in both; 48 respondents (55%) had a urethroplasty surgeon in their practice, whereas 18 (20%) had a urethroplasty surgeon within 45 minutes of his or her primary practice location. The only covariate that was associated with an increased likelihood of recommending urethroplasty in ≥ three scenarios was formal urethroplasty training. Most members (68%) reported no barriers to referring patients for urethroplasty; the most common barriers cited were long distance to urethroplasty surgeon (n 5 13, 15%) and concern about complications (n 5 8, 9%). Urethroplasty continues to be underutilized in men with anterior urethral strictures, potentially due to lack of knowledge dissemination and access to a urethroplasty surgeon. Appropriate urethroplasty utilization may increase with greater exposure to urethroplasty in training.
Keywords: Barriers; Physician practice patterns; Urethral stricture; Urethroplasty.
Figures

References
-
- Bullock TL, Brandes SB. Adult anterior urethral strictures: a national practice patterns survey of board certified urologists in the United States. J Urol. 2007;177:685–690. - PubMed
-
- Ferguson GG, Bullock TL, Anderson RE, et al. Minimally invasive methods for bulbar urethral strictures: a survey of members of the American Urological Association. Urology. 2011;78:701–706. - PubMed
-
- Rapp DE, Chanduri K, Infusino G, et al. Internet survey of management trends of urethral strictures. Urol Int. 2008;80:287–290. - PubMed
-
- Santucci RA, Joyce GF, Wise M. Male urethral stricture disease. J Urol. 2007;177:1667–1674. - PubMed
LinkOut - more resources
Full Text Sources