

Different types of white matter hyperintensities in CADASIL: Insights from 7-Tesla MRI
- PMID: 28128022
- PMCID: PMC6125962
- DOI: 10.1177/0271678X17690164
Different types of white matter hyperintensities in CADASIL: Insights from 7-Tesla MRI
Abstract
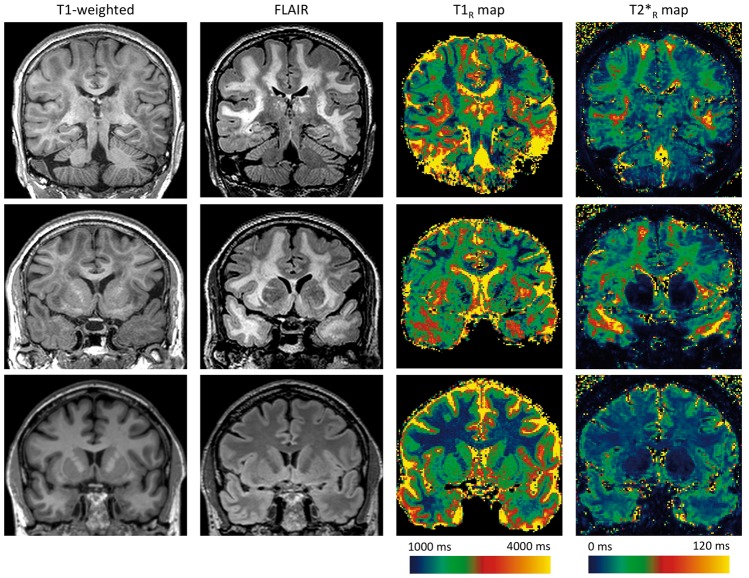
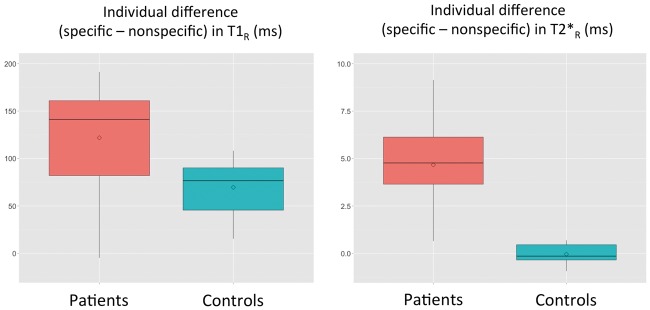
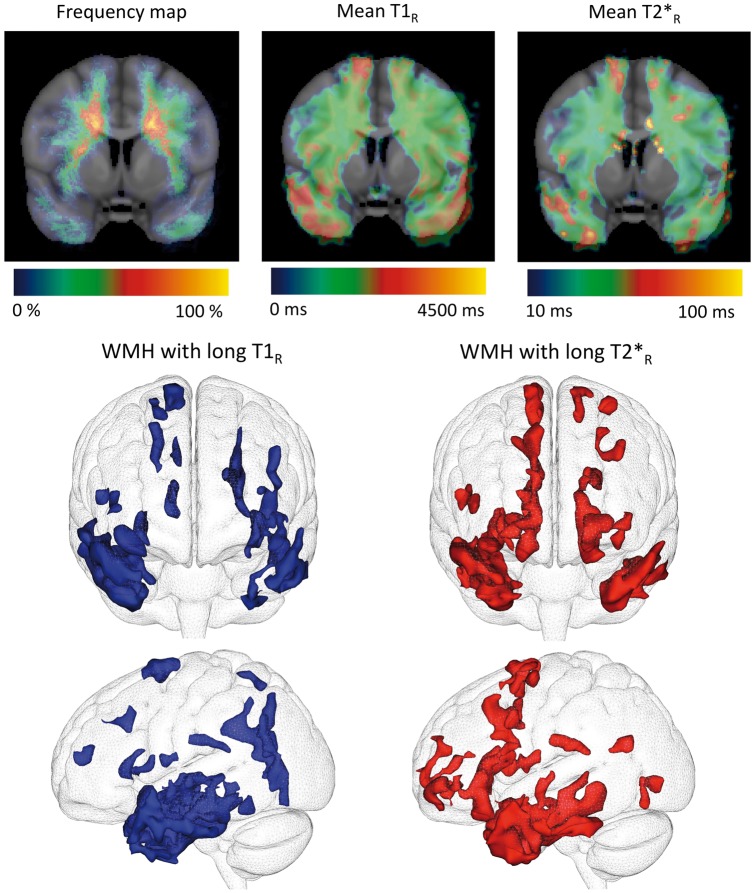
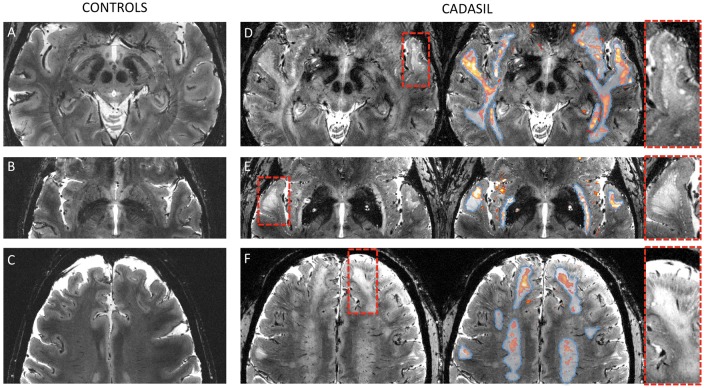
In Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL), by contrast to sporadic cerebral small vessel disease related to age and hypertension, white matter hyperintensities (WMH) are frequently observed in the white matter of anterior temporal poles, external capsules, and superior frontal regions. Whether these WMH (specific WMH) differ from those observed in other white matter areas (nonspecific WMH) remains unknown. Twenty patients were scanned to compare specific and nonspecific WMH using high-resolution images and analyses of relaxation times (T1R: longitudinal relaxation time and T2*R: effective transversal relaxation time). Specific WMH were characterized by significantly longer T1R and T2*R (T1R: 2309 ± 120 ms versus 2145 ± 138 ms; T2*R: 40 ± 5 ms versus 35 ± 5 ms, p < 0.001). These results were not explained by the presence of dilated perivascular spaces found in the close vicinity of specific WMH. They were not either explained by the normal regional variability of T1R and T2*R in the white matter nor by systematic imaging artifacts as shown by the study of 17 age- and sex-matched healthy controls. Our results suggest large differences in water content between specific and nonspecific WMH in CADASIL, supporting that mechanisms underlying WMH may differ according to their location.
Keywords: CADASIL; cerebral small vessel disease; dilated perivascular spaces; relaxometry; white matter hyperintensities.
Figures
References
-
- Chabriat H, Joutel A, Dichgans M, et al. Lancet Neurol 2009; 8: 643–653. - PubMed
-
- Auer DP, Putz B, Gossl C, et al. Differential lesion patterns in CADASIL and sporadic subcortical arteriosclerotic encephalopathy: MR imaging study with statistical parametric group comparison. Radiology 2001; 218: 443–451. - PubMed
-
- O’Sullivan M, Jarosz JM, Martin RJ, et al. MRI hyperintensities of the temporal lobe and external capsule in patients with CADASIL. Neurology 2001; 56: 628–634. - PubMed
-
- Duering M, Csanadi E, Gesierich B, et al. Incident lacunes preferentially localize to the edge of white matter hyperintensities: insights into the pathophysiology of cerebral small vessel disease. Brain 2013; 136: 2717–2726. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
