

Optimal diagnostic thresholds for diagnosis of orthostatic hypotension with a 'sit-to-stand test'
- PMID: 28129252
- PMCID: PMC5542884
- DOI: 10.1097/HJH.0000000000001265
Optimal diagnostic thresholds for diagnosis of orthostatic hypotension with a 'sit-to-stand test'
Abstract
Objective: This study aimed to identify optimal blood pressure cut-offs to diagnose orthostatic hypotension during a sit-to-stand manoeuvre.
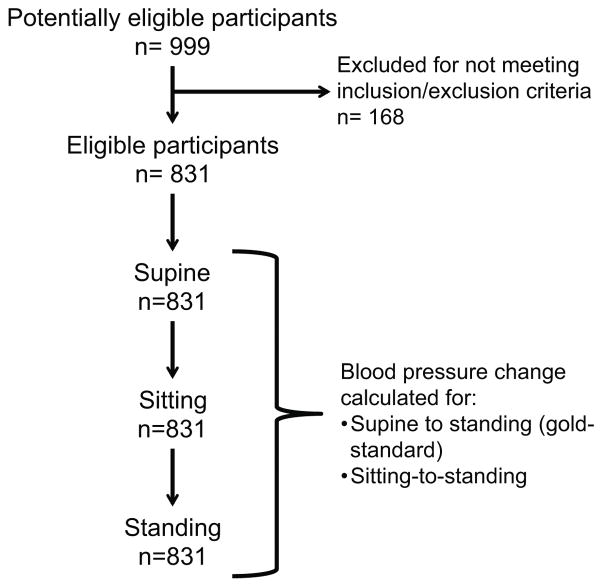
Methods: This was a cross-sectional study of patients and healthy controls from the Vanderbilt Autonomic Dysfunction Center. Blood pressure was measured while supine, seated and standing. Blood pressure changes were calculated from supine-to-standing and seated-to-standing. Orthostatic hypotension was diagnosed on the basis of a supine-to-standing SBP drop at least 20 mmHg or a DBP drop at least 10 mmHg. Receiver operator characteristic (ROC) curves identified optimal sit-to-stand cut-offs.
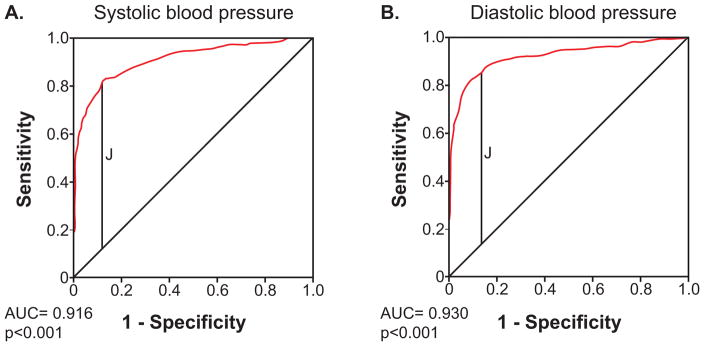
Results: Amongst the 831 individuals, more had systolic orthostatic hypotension [n = 354 (43%)] than diastolic orthostatic hypotension [n = 305 (37%)] during lying-to-standing. The ROC curves had good characteristics [SBP area under curve = 0.916 (95% confidence interval: 0.896-0.936), P < 0.001; DBP area under curve = 0.930 (95% confidence interval: 0.909-0.950), P < 0.001]. A sit-to stand SBP drop at least 15 mmHg had optimal test characteristics (sensitivity = 80.2%; specificity = 88.9%; positive predictive value = 84.2%; negative predictive value = 85.8%), as did a DBP drop at least 7 mmHg (sensitivity = 87.2%; specificity = 87.2%; positive predictive value = 80.1%; negative predictive value = 92.0%).
Conclusions: A sit-to-stand manoeuvre with lower diagnostic cut-offs for orthostatic hypotension provides a simple screening test for orthostatic hypotension in situations wherein a supine-to-standing manoeuvre cannot be easily performed. Our analysis suggests that a SBP drop at least 15 mmHg or a DBP drop at least 7 mmHg best optimizes sensitivity and specificity of this sit-to-stand test.
Figures
Comment in
-
Orthostatic hypotension: new views for an old problem.J Hypertens. 2017 May;35(5):947-949. doi: 10.1097/HJH.0000000000001272. J Hypertens. 2017. PMID: 28353545 No abstract available.
References
-
- Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. - PubMed
-
- Angelousi A, Girerd N, Benetos A, Frimat L, Gautier S, Weryha G, et al. Association between orthostatic hypotension and cardiovascular risk, cerebrovascular risk, cognitive decline and falls as well as overall mortality: a systematic review and meta-analysis. J Hypertens. 2014;32(8):1562–1571. discussion 1571. - PubMed
-
- Ricci F, Fedorowski A, Radico F, Romanello M, Tatasciore A, Di Nicola M, et al. Cardiovascular morbidity and mortality related to orthostatic hypotension: a meta-analysis of prospective observational studies. Eur Heart J. 2015;36(25):1609–1617. - PubMed
-
- Veronese N, De Rui M, Bolzetta F, Zambon S, Corti MC, Baggio G, et al. Orthostatic Changes in Blood Pressure and Mortality in the Elderly: The Pro.V. A Study. American Journal of Hypertension. 2015;28(10):1248–1256. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
