

Regionally Specific Brain Volumetric and Cortical Thickness Changes in HIV-Infected Patients in the HAART Era
- PMID: 28129254
- PMCID: PMC5340610
- DOI: 10.1097/QAI.0000000000001294
Regionally Specific Brain Volumetric and Cortical Thickness Changes in HIV-Infected Patients in the HAART Era
Abstract
Background: Cognitive impairment still occurs in a substantial subset of HIV-infected patients, despite effective viral suppression with highly active antiretroviral therapy (HAART). Structural brain changes may provide clues about the underlying pathophysiology. This study provides a detailed spatial characterization of the pattern and extent of brain volume changes associated with HIV and relates these brain measures to cognitive ability and clinical variables.
Methods: Multiple novel neuroimaging techniques (deformation-based morphometry, voxel-based morphometry, and cortical modeling) were used to assess regional brain volumes in 125 HIV-infected patients and 62 HIV-uninfected individuals. Ninety percent of the HIV-infected patients were on stable HAART with most of them (75%) having plasma viral suppression. Brain volumetrics and cortical thickness estimates were compared between the HIV-infected and uninfected groups, and the relationships between these measures of brain volume and indices of current and past infection severity, central nervous system penetration of HAART, and cognitive performance were assessed.
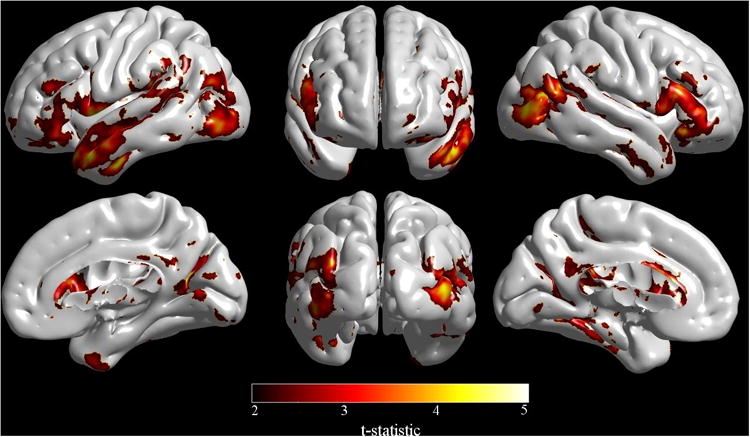
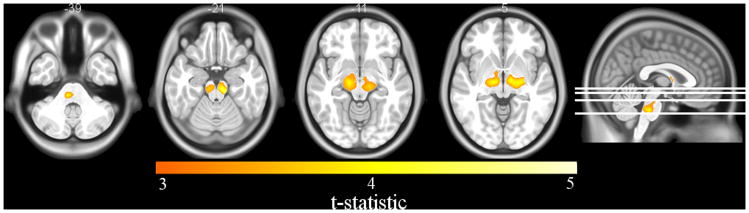
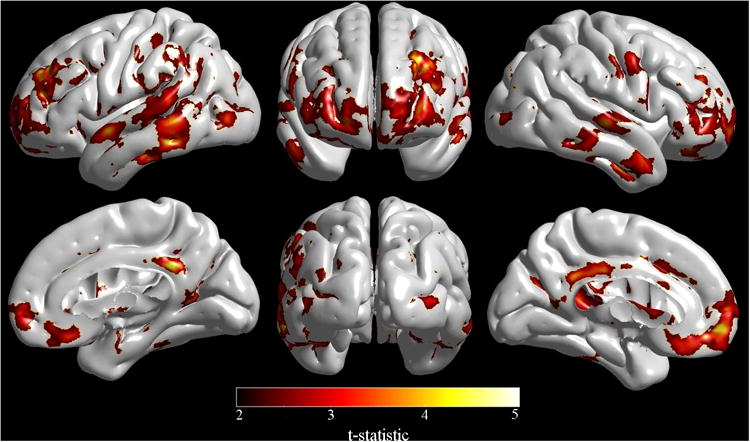
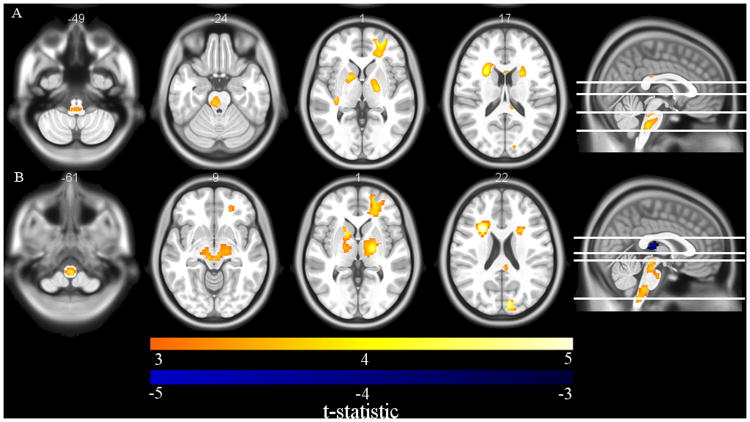
Results: Regionally specific patterns of reduced thalamic and brainstem volumes and reduced cortical thickness in the orbitofrontal cortex, cingulate gyrus, primary motor and sensory cortex, temporal, and frontal lobes were seen in HIV-infected patients compared to HIV-uninfected participants. Observed white matter loss and subcortical atrophy were associated with lower nadir CD4 cell counts, while reduction in cortical thickness was related to worse cognitive performance.
Conclusions: Our findings suggest that distinct mechanisms may underlie cortical and subcortical injury in people with HIV and argues for the potential importance of early initiation of HAART to protect long-term brain health.
Conflict of interest statement
Figures
References
-
- Mothobi NZ, Brew BJ. Neurocognitive dysfunction in highly active antiretroviral therapy era. Curr Opin Infect Dis. 2012;25(1):4–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
