

Chlamydia trachomatis Pgp3 Antibody Population Seroprevalence before and during an Era of Widespread Opportunistic Chlamydia Screening in England (1994-2012)
- PMID: 28129328
- PMCID: PMC5271337
- DOI: 10.1371/journal.pone.0152810
Chlamydia trachomatis Pgp3 Antibody Population Seroprevalence before and during an Era of Widespread Opportunistic Chlamydia Screening in England (1994-2012)
Abstract
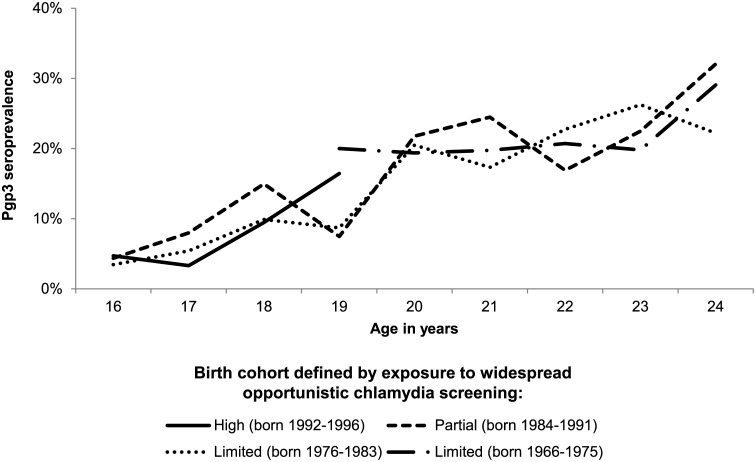
Background: Opportunistic chlamydia screening of <25 year-olds was nationally-implemented in England in 2008 but its impact on chlamydia transmission is poorly understood. We undertook a population-based seroprevalence study to explore the impact of screening on cumulative incidence of chlamydia, as measured by C.trachomatis-specific antibody.
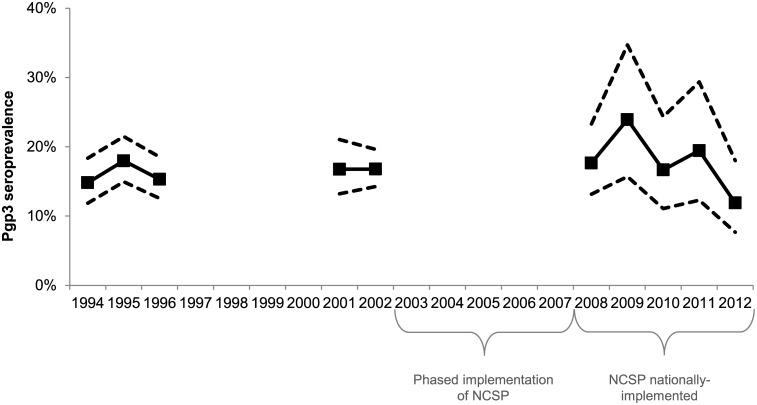
Methods: Anonymised sera from participants in the nationally-representative Health Surveys for England (HSE) were tested for C.trachomatis antibodies using two novel Pgp3 enzyme-linked immunosorbent assays (ELISAs) as a marker of past infection. Determinants of being seropositive were explored using logistic regression among 16-44 year-old women and men in 2010 and 2012 (years when sexual behaviour questions were included in the survey) (n = 1,402 women; 1,119 men). Seroprevalence trends among 16-24 year-old women (n = 3,361) were investigated over ten time points from 1994-2012.
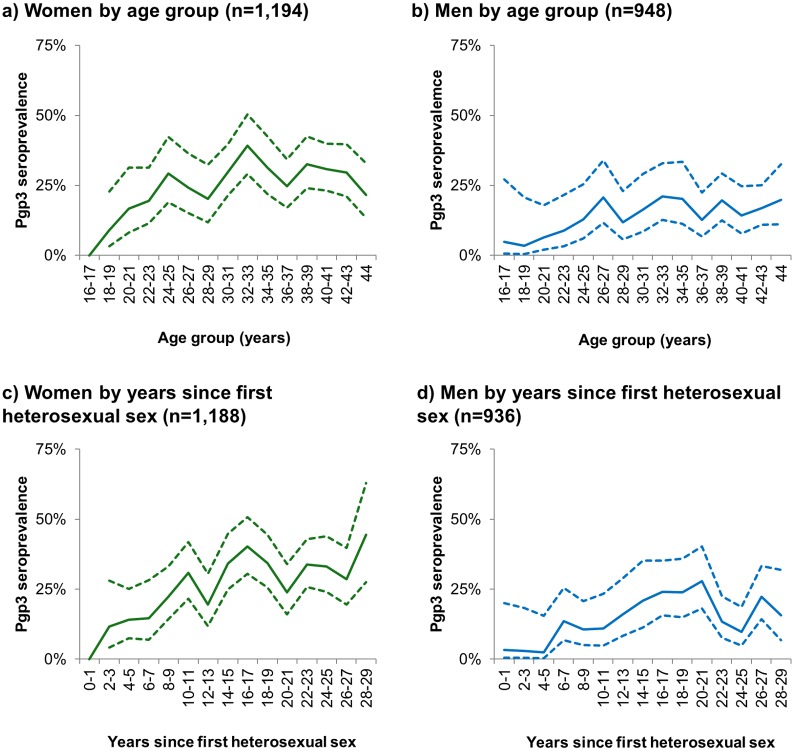
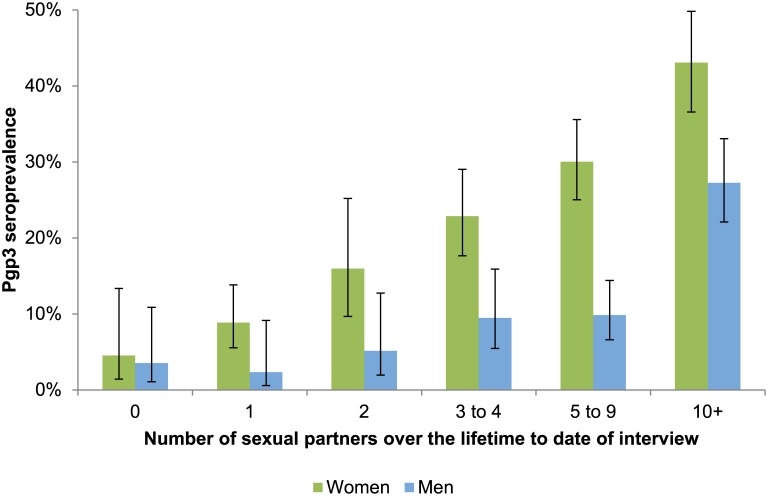
Results: In HSE2010/2012, Pgp3 seroprevalence among 16-44 year-olds was 24.4% (95%CI 22.0-27.1) in women and 13.9% (11.8-16.2) in men. Seroprevalence increased with age (up to 33.5% [27.5-40.2] in 30-34 year-old women, 18.7% [13.4-25.6] in 35-39 year-old men); years since first sex; number of lifetime sexual partners; and younger age at first sex. 76.7% of seropositive 16-24 year-olds had never been diagnosed with chlamydia. Among 16-24 year-old women, a non-significant decline in seroprevalence was observed from 2008-2012 (prevalence ratio per year: 0.94 [0.84-1.05]).
Conclusion: Our application of Pgp3 ELISAs demonstrates a high lifetime risk of chlamydia infection among women and a large proportion of undiagnosed infections. A decrease in age-specific cumulative incidence following national implementation of opportunistic chlamydia screening has not yet been demonstrated. We propose these assays be used to assess impact of chlamydia control programmes.
Conflict of interest statement
SCW, AN and GM are employed by Public Health England. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Public Health England. Table 8: Number and rates of selected STI diagnoses in the UK, 2008–2012. 2014. 2014.
-
- Gottlieb SL, Martin DH, Xu F, Byrne GI, Brunham RC. Summary: The natural history and immunobiology of Chlamydia trachomatis genital infection and implications for Chlamydia control. J Infect Dis 2010. June 15;201 Suppl 2:S190–S204. - PubMed
-
- Westrom L, Joesoef R, Reynolds G, Hagdu A, Thompson SE. Pelvic inflammatory disease and fertility. A cohort study of 1,844 women with laparoscopically verified disease and 657 control women with normal laparoscopic results. Sex Transm Dis 1992. July;19(4):185–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
