

Long-term functional outcome in patients with acquired infections after acute spinal cord injury
- PMID: 28130472
- PMCID: PMC5331871
- DOI: 10.1212/WNL.0000000000003652
Long-term functional outcome in patients with acquired infections after acute spinal cord injury
Abstract
Objective: To investigate whether prevalent hospital-acquired pneumonia and wound infection affect the clinical long-term outcome after acute traumatic spinal cord injury (SCI).
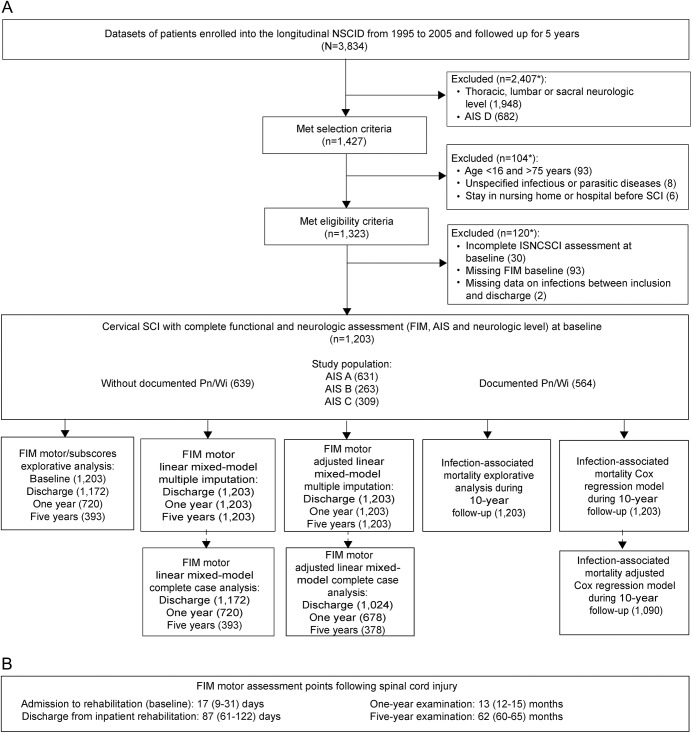
Methods: This was a longitudinal cohort study within the prospective multicenter National Spinal Cord Injury Database (Birmingham, Alabama). We screened datasets of 3,834 patients enrolled in 20 trial centers from 1995 to 2005 followed up until 2016. Eligibility criteria were cervical SCI and American Spinal Cord Injury Association impairment scale A, B, and C. Pneumonia or postoperative wound infections (Pn/Wi) acquired during acute medical care/inpatient rehabilitation were analyzed for their association with changes in the motor items of the Functional Independence Measure (FIMmotor) using regression models (primary endpoint 5-year follow-up). Pn/Wi-related mortality was assessed as a secondary endpoint (10-year follow-up).
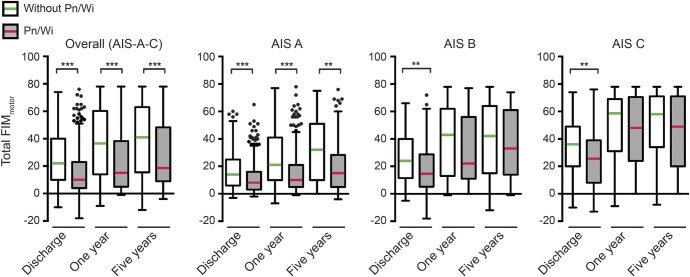
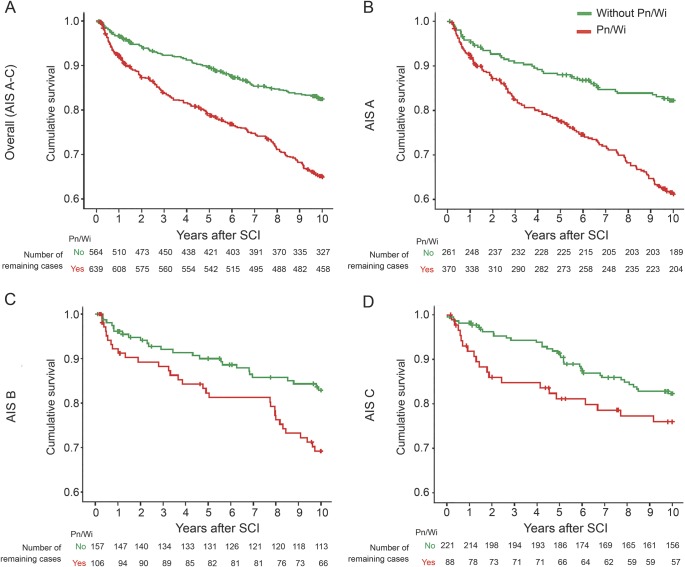
Results: A total of 1,203 patients met the eligibility criteria. During hospitalization, 564 patients (47%) developed Pn/Wi (pneumonia n = 540; postoperative wound infection n = 11; pneumonia and postoperative wound infection n = 13). Adjusted linear mixed models after multiple imputation revealed that Pn/Wi are significantly associated with lower gain in FIMmotor up to 5 years after SCI (-7.4 points, 95% confidence interval [CI] -11.5 to -3.3). Adjusted Cox regression identified Pn/Wi as a highly significant risk factor for death up to 10 years after SCI (hazard ratio 1.65, 95% CI 1.26 to 2.16).
Conclusion: Hospital-acquired Pn/Wi are predictive of propagated disability and mortality after SCI. Pn/Wi qualify as a potent and targetable outcome-modifying factor. Pn/Wi prevention constitutes a viable strategy to protect functional recovery and reduce mortality. Pn/Wi can be considered as rehabilitation confounders in clinical trials.
© 2017 American Academy of Neurology.
Figures
Comment in
-
Journal Club: Long-term functional outcome in patients with acquired infections after acute spinal cord injury.Neurology. 2017 Aug 15;89(7):e76-e78. doi: 10.1212/WNL.0000000000004241. Neurology. 2017. PMID: 28808174 Free PMC article. No abstract available.
References
-
- Dietz V, Curt A. Translating preclinical approaches into human application. Handb Clin Neurol 2012;109:399–409. - PubMed
-
- Siddiqui AM, Khazaei M, Fehlings MG. Translating mechanisms of neuroprotection, regeneration, and repair to treatment of spinal cord injury. Prog Brain Res 2015;218:15–54. - PubMed
-
- Curt A, Van Hedel HJ, Klaus D, Dietz V, EM-SCI Study Group. Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. J Neurotrauma 2008;25:677–685. - PubMed
-
- Fawcett JW, Curt A, Steeves JD, et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2007;45:190–205. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous