

3D late gadolinium enhanced cardiovascular MR with CENTRA-PLUS profile/view ordering: Feasibility of right ventricular myocardial damage assessment using a swine animal model
- PMID: 28131907
- PMCID: PMC5410402
- DOI: 10.1016/j.mri.2017.01.015
3D late gadolinium enhanced cardiovascular MR with CENTRA-PLUS profile/view ordering: Feasibility of right ventricular myocardial damage assessment using a swine animal model
Abstract
Aims: To develop a high-resolution, 3D late gadolinium enhancement (LGE) cardiovascular magnetic resonance imaging (MRI) technique for improved assessment of myocardial scars, and evaluate its performance against 2D breath-held (BH) LGE MRI using a surgically implanted animal scar model in the right ventricle (RV).
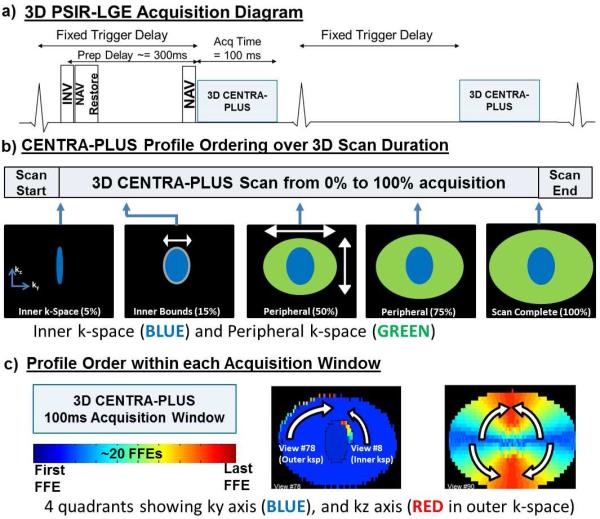
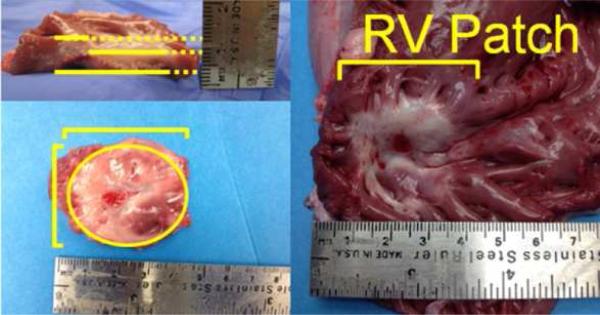
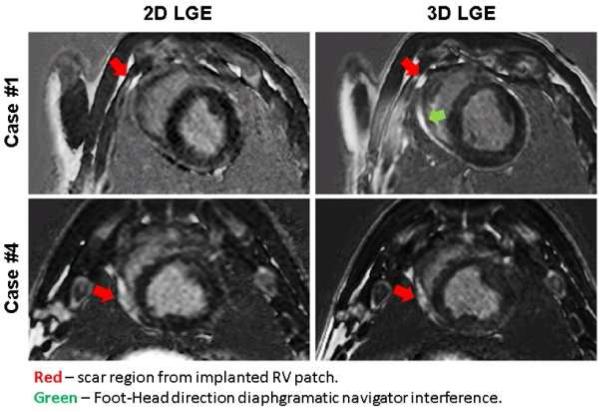
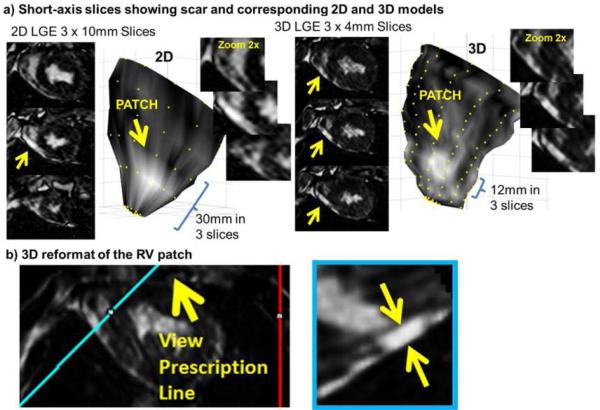
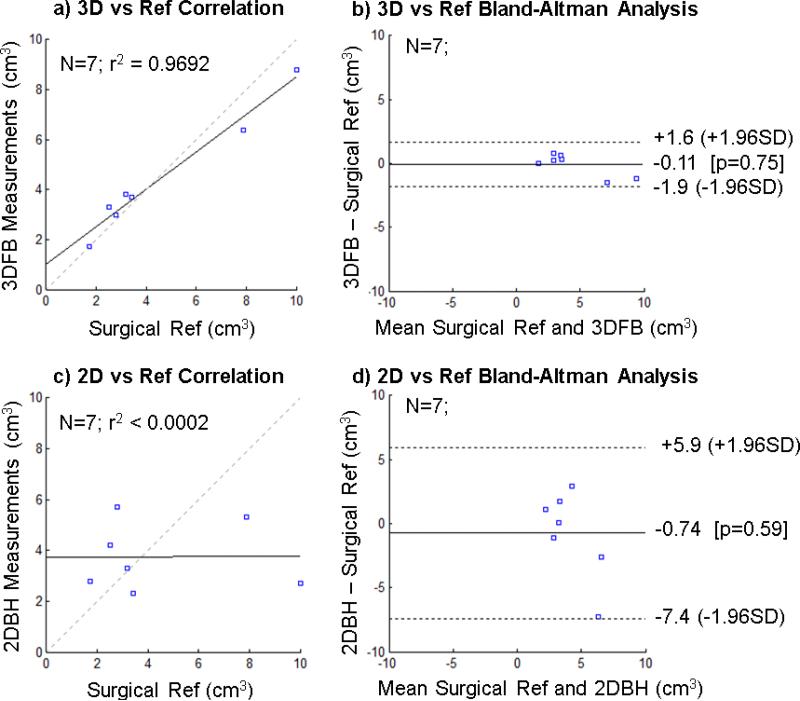
Methods and results: A k-space segmented 3D LGE acquisition using CENTRA-PLUS (Contrast ENhanced Timing Robust Acquisition with Preparation of LongitUdinal Signal; or CP) ordering is proposed. 8 pigs were surgically prepared with cardiac patch implantation in the RV, followed in 60days by 1.5T MRI. LGE with Phase-Sensitive Inversion Recovery (PSIR) were performed as follows: 1) 2DBH using pneumatic control, and 2) navigator-gated, 3D free-breathing (3DFB)-CP-LGE with slice-tracking. The animal heart was excised immediately after cardiac MR for scar volume quantification. RV scar volumes were also delineated from the 2DBH and 3DFB-CP-LGE images for comparison against the surgical standard. Apparent scar/normal tissue signal-to-noise ratio (aSNR) and contrast-to-noise ratio (aCNR) were also calculated. 3DFB-CP-LGE technique was successfully performed in all animals. No difference in aCNR was noted, but aSNR was significantly higher using the 3D technique (p<0.05). Against the surgical reference volume, the 3DFB-CP-LGE-derived delineation yielded significantly less volume quantification error compared to 2DBH-derived volumes (15±10% vs 55±33%; p<0.05).
Conclusion: Compared to conventional 2DBH-LGE, 3DFB-LGE acquisition using CENTRA-PLUS provided superior scar volume quantification and improved aSNR.
Keywords: Breath-hold; Late gadolinium enhancement MRI; Myocardial infarction; Navigator; Viability imaging.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Feasibility study of a single breath-hold, 3D mDIXON pulse sequence for late gadolinium enhancement imaging of ischemic scar.J Magn Reson Imaging. 2019 May;49(5):1437-1445. doi: 10.1002/jmri.26519. Epub 2018 Dec 31. J Magn Reson Imaging. 2019. PMID: 30597661
-
Improved border sharpness of post-infarct scar by a novel self-navigated free-breathing high-resolution 3D whole-heart inversion recovery magnetic resonance approach.Int J Cardiovasc Imaging. 2016 Dec;32(12):1735-1744. doi: 10.1007/s10554-016-0963-4. Epub 2016 Aug 22. Int J Cardiovasc Imaging. 2016. PMID: 27549804
-
Three-dimensional phase-sensitive inversion recovery sequencing in the evaluation of left ventricular myocardial scars in ischemic and non-ischemic cardiomyopathy: comparison to three-dimensional inversion recovery sequencing.Eur J Radiol. 2014 Dec;83(12):2159-2166. doi: 10.1016/j.ejrad.2014.09.014. Epub 2014 Sep 30. Eur J Radiol. 2014. PMID: 25311877
-
Whole-Heart High-Resolution Late Gadolinium Enhancement: Techniques and Clinical Applications.J Magn Reson Imaging. 2022 Apr;55(4):967-987. doi: 10.1002/jmri.27732. Epub 2021 Jun 21. J Magn Reson Imaging. 2022. PMID: 34155715 Free PMC article. Review.
-
[Cardiac magnetic resonance imaging and the myocardium : Differentiation between vital and nonvital tissue].Herzschrittmacherther Elektrophysiol. 2022 Sep;33(3):272-277. doi: 10.1007/s00399-022-00874-8. Epub 2022 Jul 4. Herzschrittmacherther Elektrophysiol. 2022. PMID: 35781833 Review. German.
Cited by
-
An Improved 3D Deep Learning-Based Segmentation of Left Ventricular Myocardial Diseases from Delayed-Enhancement MRI with Inclusion and Classification Prior Information U-Net (ICPIU-Net).Sensors (Basel). 2022 Mar 8;22(6):2084. doi: 10.3390/s22062084. Sensors (Basel). 2022. PMID: 35336258 Free PMC article.
-
Accelerated high-resolution free-breathing 3D whole-heart T2-prepared black-blood and bright-blood cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2020 Dec 14;22(1):88. doi: 10.1186/s12968-020-00691-3. J Cardiovasc Magn Reson. 2020. PMID: 33317570 Free PMC article.
References
-
- Kim RJ, Fieno DS, Parrish TB, et al. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100(19):1992–2002. - PubMed
-
- Fieno DS, Kim RJ, Chen EL, Lomasney JW, Klocke FJ, Judd RM. Contrast-enhanced magnetic resonance imaging of myocardium at risk: distinction between reversible and irreversible injury throughout infarct healing. Journal of the American College of Cardiology. 2000;36(6):1985–1991. - PubMed
-
- Klein C, Nekolla SG, Bengel FM, et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation. 2002;105(2):162–167. - PubMed
-
- Wagner A, Mahrholdt H, Holly TA, et al. Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet. 2003;361(9355):374–379. - PubMed
-
- Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445–1453. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
