

Tibial condylar valgus osteotomy (TCVO) for osteoarthritis of the knee: 5-year clinical and radiological results
- PMID: 28132085
- PMCID: PMC5310550
- DOI: 10.1007/s00402-016-2609-3
Tibial condylar valgus osteotomy (TCVO) for osteoarthritis of the knee: 5-year clinical and radiological results
Abstract
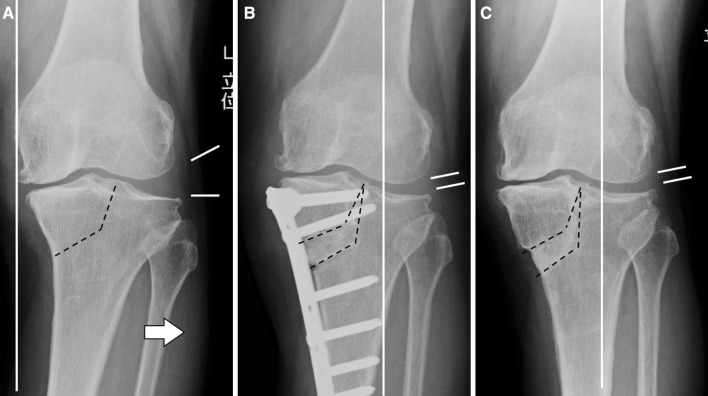
Purpose: Tibial condylar valgus osteotomy (TCVO) is a type of opening-wedge high tibial osteotomy for advanced medial knee osteoarthritis (OA) with subluxated lateral joint. We report the concept, the current surgical technique with a locking plate, and the short-term clinical and radiological results of this procedure.
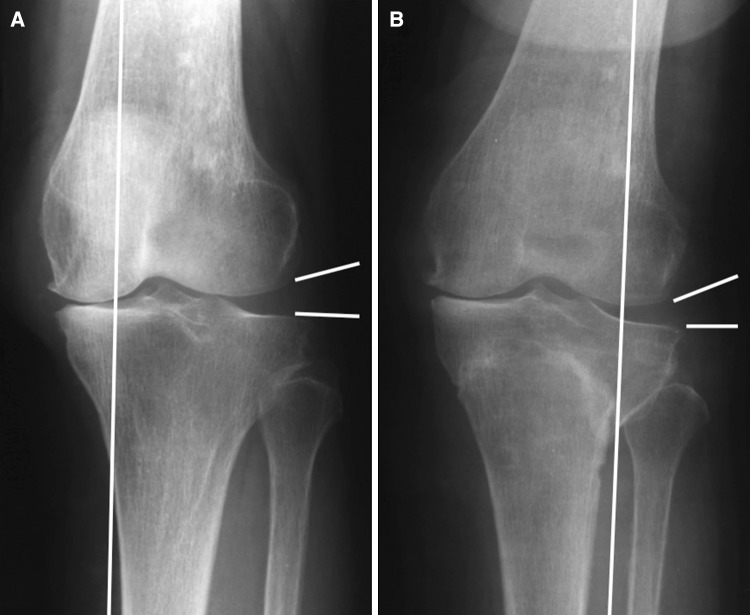
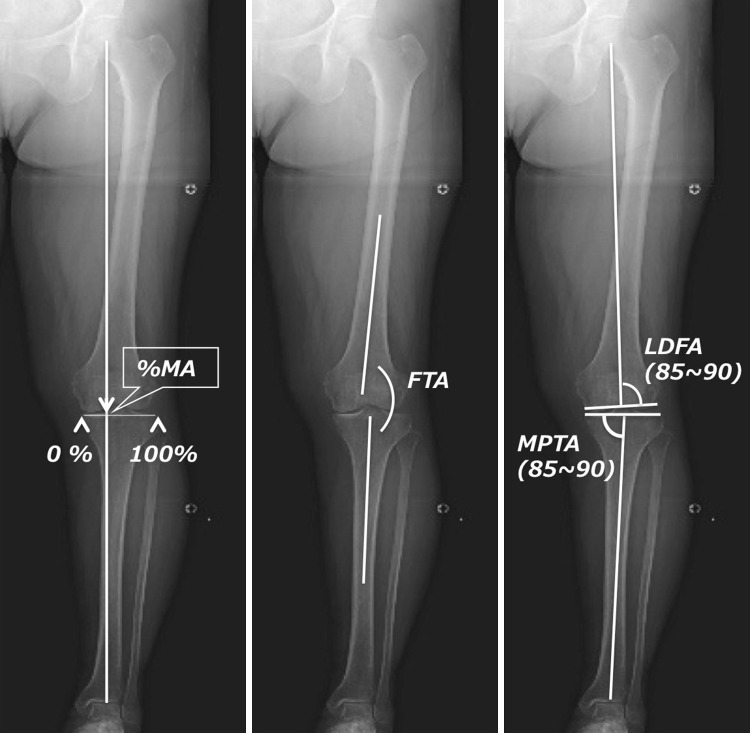
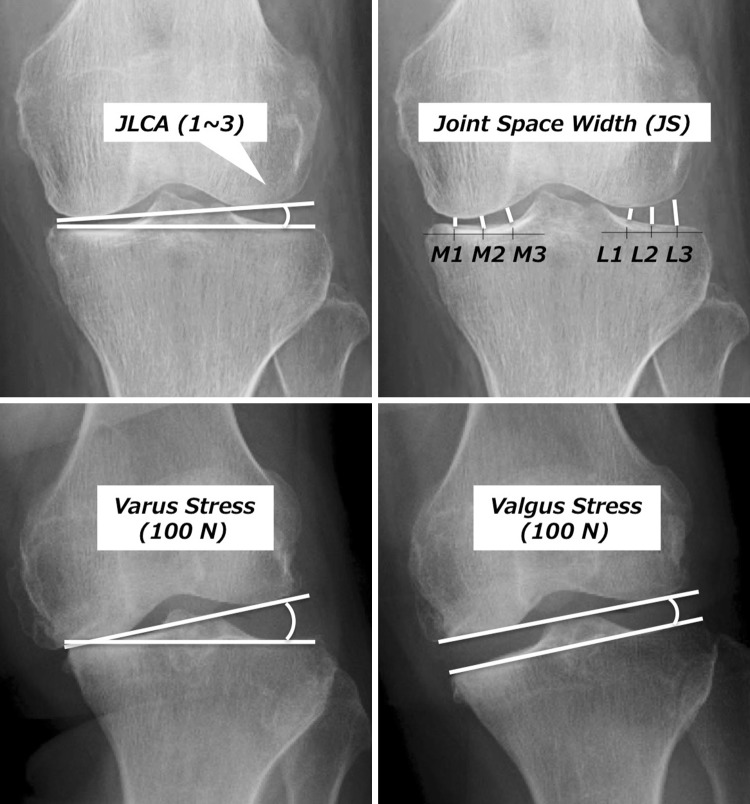
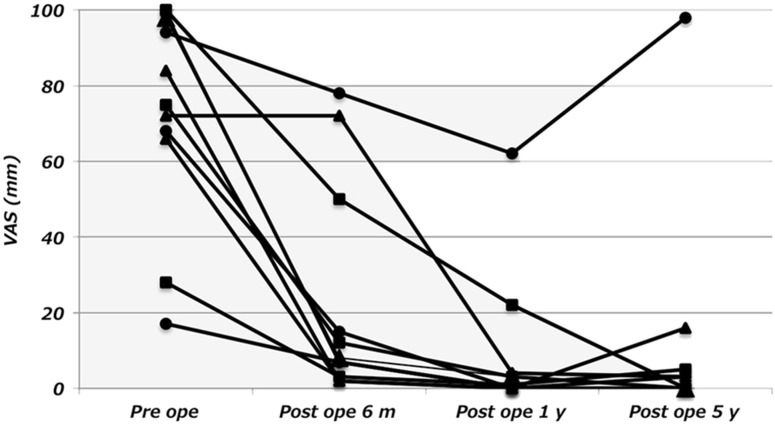
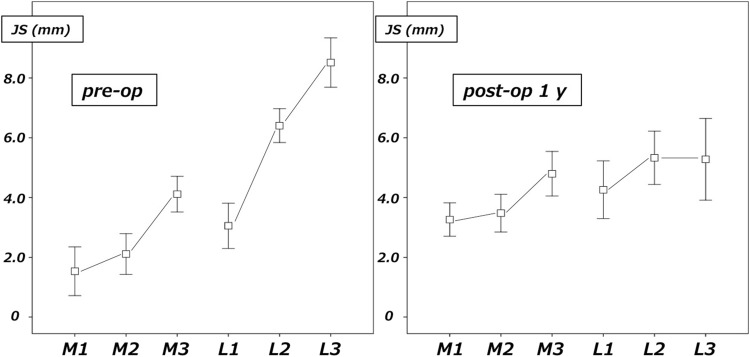
Methods: 11 knees with medial OA and a widened lateral joint were treated by TCVO (KL stage III: 6, IV: 5). In this procedure, by the L-shaped osteotomy from the medial side of the proximal tibia to the intercondylar eminence and the valgus correction, lateralization of the mechanical axis and reduction of the subluxated lateral joint are obtained with early postoperative weight-bearing. Before, 6 months, 1, and 5 years after the operation, a visual analog scale (VAS), the Western Ontario and McMaster Universities Arthritis Index (WOMAC), alignment of the lower extremity, and congruency and stability of the femorotibial joint were investigated.
Results: The VAS improved from an average of 73 mm to 13 mm, and the total WOMAC score from 52 to 14 before to 5 years after the operation, respectively. The mechanical axis changed from 1 to 60%, and the FTA changed from 186° to 171°. The joint line convergence angle (JLCA) changed from 6° to 1°, and the angle difference of JLCA between varus and valgus stress improved from 8° to 4° after the procedure.
Conclusion: Improvements in pain and activities of daily living were observed by TCVO along with valgus correction of the lower extremity and stabilization of the femorotibial joint.
Keywords: High tibial osteotomy; Osteoarthritis of the knee; Tibial condylar valgus osteotomy.
Conflict of interest statement
None.
Figures
Similar articles
-
Salvage of severe knee osteoarthritis: efficacy of tibial condylar valgus osteotomy versus open wedge high tibial osteotomy.J Orthop Surg Res. 2021 Jul 14;16(1):451. doi: 10.1186/s13018-021-02597-x. J Orthop Surg Res. 2021. PMID: 34261504 Free PMC article.
-
A case series of lateral opening wedge high tibial osteotomy for valgus malalignment.Knee Surg Sports Traumatol Arthrosc. 2013 Jan;21(1):152-60. doi: 10.1007/s00167-012-2070-y. Epub 2012 Jun 17. Knee Surg Sports Traumatol Arthrosc. 2013. PMID: 22706968 Clinical Trial.
-
Early weight bearing versus delayed weight bearing in medial opening wedge high tibial osteotomy: a randomized controlled trial.Knee Surg Sports Traumatol Arthrosc. 2017 Dec;25(12):3670-3678. doi: 10.1007/s00167-016-4225-8. Epub 2016 Jul 1. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27371292 Clinical Trial.
-
Tibial condylar valgus osteotomy - indications and technique.J Exp Orthop. 2020 May 13;7(1):30. doi: 10.1186/s40634-020-00247-5. J Exp Orthop. 2020. PMID: 32405777 Free PMC article. Review.
-
Intra- and Extra-Articular Deformity of Lower Limb: Tibial Condylar Valgus Osteotomy (TCVO) and Distal Tibial Oblique Osteotomy (DTOO) for Reconstruction of Joint Congruency.Adv Orthop. 2019 Feb 18;2019:8605674. doi: 10.1155/2019/8605674. eCollection 2019. Adv Orthop. 2019. PMID: 30906598 Free PMC article. Review.
Cited by
-
Comparison of radiological features of high tibial osteotomy and tibial condylar valgus osteotomy.BMC Musculoskelet Disord. 2019 Sep 4;20(1):409. doi: 10.1186/s12891-019-2764-0. BMC Musculoskelet Disord. 2019. PMID: 31484580 Free PMC article.
-
The influence of post-operative knee coronal alignment parameters on long-term patient-reported outcomes after closed-wedge high tibial osteotomy.J Orthop. 2020 Jan 29;20:177-180. doi: 10.1016/j.jor.2020.01.042. eCollection 2020 Jul-Aug. J Orthop. 2020. PMID: 32025144 Free PMC article.
-
Tibial condylar valgus osteotomy for the treatment of intra-articular varus deformity of the knee.Ann Jt. 2022 Oct 15;7:37. doi: 10.21037/aoj-22-19. eCollection 2022. Ann Jt. 2022. PMID: 38529161 Free PMC article. Review.
-
Tibial Condyle Valgus Osteotomy for Ipsilateral Knee Osteoarthritis after Hip Arthrodesis.Case Rep Orthop. 2021 Oct 29;2021:6443618. doi: 10.1155/2021/6443618. eCollection 2021. Case Rep Orthop. 2021. PMID: 34745676 Free PMC article.
-
Tibial condylar valgus osteotomy (TCVO): Surgical technique and clinical results for knee osteoarthritis with varus deformity.J Clin Orthop Trauma. 2021 Sep 7;22:101589. doi: 10.1016/j.jcot.2021.101589. eCollection 2021 Nov. J Clin Orthop Trauma. 2021. PMID: 34540585 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
