

Factors affecting dental biofilm in patients wearing fixed orthodontic appliances
- PMID: 28133715
- PMCID: PMC5276803
- DOI: 10.1186/s40510-016-0158-5
Factors affecting dental biofilm in patients wearing fixed orthodontic appliances
Abstract
Background: The aim of this study is to investigate the amount and the distribution of biofilm in patients wearing fixed appliances and its relation with age, gender, frequency of tooth brushing, and patient motivation.
Methods: The sample comprised 52 patients (15.5 ± 3.6 years old, 30 females and 22 males) wearing fixed orthodontic appliances. Dental biofilm was assessed using a modified plaque index (PI). A questionnaire was used to collect patient's information, including gender, age, treatment motivation, and frequency of tooth brushing.
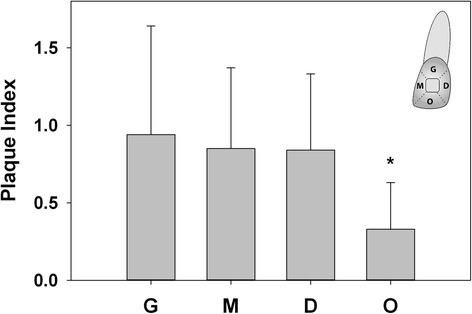
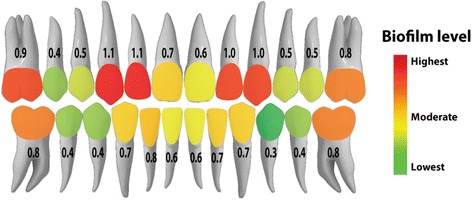
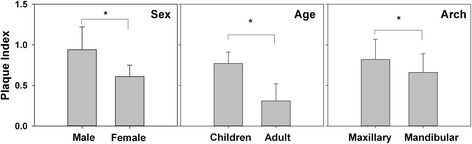
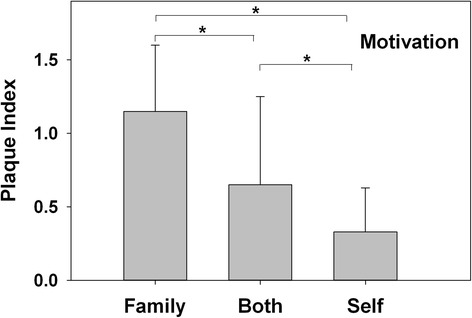
Results: Gingival (PI score = 0.9 ± 0.7), mesial (0.8 ± 0.6), and distal (0.8 ± 0.5) areas accumulated more biofilm than occlusal areas (0.3 ± 0.3) (P < 0.038). The maxillary lateral incisors (1.1 ± 0.8) and maxillary canines (1.0 ± 0.8) had more biofilm than other teeth (P < 0.05). The maxillary arch (0.8 ± 0.7) had significantly more biofilm than mandibular arch (0.6 ± 0.6) (P = 0.042). No significant difference was found between the right side (0.7 ± 0.7) and left side (0.7 ± 0.6) (P = 0.627). Less biofilm was found in females (0.6 ± 0.5), adults (0.3 ± 0.3), and "self-motivated" patients (0.3 ± 0.3), compared with males (0.9 ± 0.5), children (0.8 ± 0.6), and "family-motivated" patients (1.1 ± 0.5) (P < 0.001). The amount of biofilm was associated with self-report of the frequency of daily tooth brushing (P < 0.001).
Conclusions: Patients wearing fixed orthodontic appliances have the highest biofilm accumulation on the maxillary lateral incisors and maxillary canines, particularly in the gingival area and areas behind arch wires. Less biofilm was observed in female and adult patients and in those who were self-motivated and brushed their teeth more often.
Keywords: Biofilm; Dental plaque; Oral hygiene; Orthodontics; White spot lesions.
Figures

Similar articles
-
An orthodontic tooth brushing technique to enhance oral hygiene in patients wearing fixed orthodontic appliances: A randomized controlled trial.Int J Dent Hyg. 2023 Aug;21(3):634-640. doi: 10.1111/idh.12686. Epub 2023 Apr 27. Int J Dent Hyg. 2023. PMID: 37103919 Clinical Trial.
-
Age and gender influence on oral hygiene among adolescents with fixed orthodontic appliances.Stomatologija. 2016;18(2):61-5. Stomatologija. 2016. PMID: 27649721
-
Changes in the supragingival microbiota surrounding brackets of upper central incisors during orthodontic treatment.Acta Odontol Scand. 2013 Nov;71(6):1547-54. doi: 10.3109/00016357.2013.776107. Acta Odontol Scand. 2013. PMID: 24180590
-
[White spot lesions and orthodontic treatment. Prevention and treatment].Orthod Fr. 2014 Sep;85(3):235-44. doi: 10.1051/orthodfr/2014016. Epub 2014 Aug 28. Orthod Fr. 2014. PMID: 25158746 Review. French.
-
[Mechanism and risk factors of oral biofilm formation].Postepy Hig Med Dosw (Online). 2013 Aug 2;67:736-41. doi: 10.5604/17322693.1061393. Postepy Hig Med Dosw (Online). 2013. PMID: 24018439 Review. Polish.
Cited by
-
Assessment of Motivations, Treatment Risks, and Oral Health in Adults with Fixed Orthodontic Care: A Cross-Sectional Study.Medicina (Kaunas). 2024 Jul 17;60(7):1149. doi: 10.3390/medicina60071149. Medicina (Kaunas). 2024. PMID: 39064578 Free PMC article.
-
Tooth mousse containing casein phosphopeptide-amorphous calcium phosphate prevents biofilm formation of Streptococcus mutans.BMC Oral Health. 2021 Mar 19;21(1):136. doi: 10.1186/s12903-021-01502-6. BMC Oral Health. 2021. PMID: 33740976 Free PMC article.
-
Gingival proliferative growth - stress and cytoarchitecture related with fixed and mobile orthodontic therapy.Rom J Morphol Embryol. 2020 Oct-Dec;61(4):1287-1294. doi: 10.47162/RJME.61.4.29. Rom J Morphol Embryol. 2020. PMID: 34171076 Free PMC article.
-
Oral antiseptics and nickel-titanium alloys: mechanical and chemical effects of interaction.Odontology. 2019 Apr;107(2):150-157. doi: 10.1007/s10266-018-0387-9. Epub 2018 Sep 3. Odontology. 2019. PMID: 30178177
-
Long-term changes in thickness, live/dead bacterial ratio, and mineral content in biofilm on ceramic and stainless steel orthodontic attachments.J Orofac Orthop. 2023 Oct;84(Suppl 3):251-258. doi: 10.1007/s00056-023-00452-8. Epub 2023 Feb 23. J Orofac Orthop. 2023. PMID: 36820892 English.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
