

Typical and atypical pathology in primary progressive aphasia variants
- PMID: 28133816
- PMCID: PMC5421819
- DOI: 10.1002/ana.24885
Typical and atypical pathology in primary progressive aphasia variants
Abstract
Objective: To characterize in vivo signatures of pathological diagnosis in a large cohort of patients with primary progressive aphasia (PPA) variants defined by current diagnostic classification.
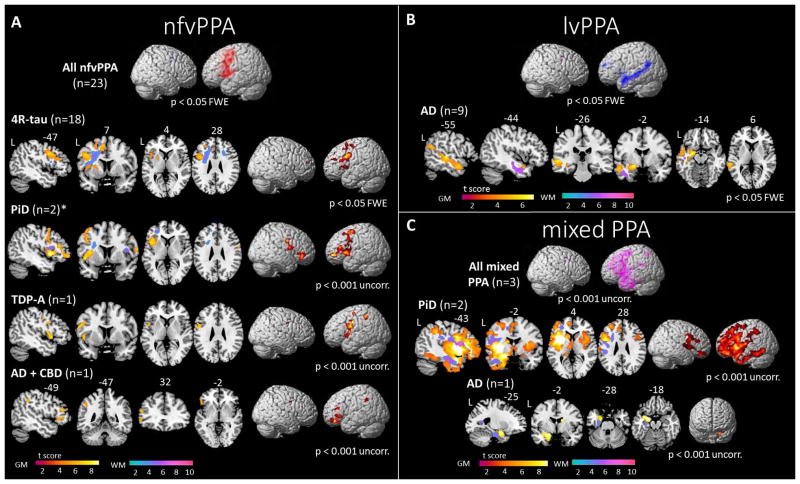
Methods: Extensive clinical, cognitive, neuroimaging, and neuropathological data were collected from 69 patients with sporadic PPA, divided into 29 semantic (svPPA), 25 nonfluent (nfvPPA), 11 logopenic (lvPPA), and 4 mixed PPA. Patterns of gray matter (GM) and white matter (WM) atrophy at presentation were assessed and tested as predictors of pathological diagnosis using support vector machine (SVM) algorithms.
Results: A clinical diagnosis of PPA was associated with frontotemporal lobar degeneration (FTLD) with transactive response DNA-binding protein (TDP) inclusions in 40.5%, FTLD-tau in 40.5%, and Alzheimer disease (AD) pathology in 19% of cases. Each variant was associated with 1 typical pathology; 24 of 29 (83%) svPPA showed FTLD-TDP type C, 22 of 25 (88%) nfvPPA showed FTLD-tau, and all 11 lvPPA had AD. Within FTLD-tau, 4R-tau pathology was commonly associated with nfvPPA, whereas Pick disease was observed in a minority of subjects across all variants except for lvPPA. Compared with pathologically typical cases, svPPA-tau showed significant extrapyramidal signs, greater executive impairment, and severe striatal and frontal GM and WM atrophy. nfvPPA-TDP patients lacked general motor symptoms or significant WM atrophy. Combining GM and WM volumes, SVM analysis showed 92.7% accuracy to distinguish FTLD-tau and FTLD-TDP pathologies across variants.
Interpretation: Each PPA clinical variant is associated with a typical and most frequent cognitive, neuroimaging, and neuropathological profile. Specific clinical and early anatomical features may suggest rare and atypical pathological diagnosis in vivo. Ann Neurol 2017;81:430-443.
© 2017 American Neurological Association.
Conflict of interest statement
Nothing to report.
Figures




References
-
- Chare L, Hodges JR, Leyton CE, et al. New criteria for frontotemporal dementia syndromes: clinical and pathological diagnostic implications. Journal of neurology, neurosurgery, and psychiatry. 2014 Aug;85(8):865–70. - PubMed
MeSH terms
Substances
Grants and funding
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- P01 AG017586/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- U01 AG052943/AG/NIA NIH HHS/United States
- K23 AG048291/AG/NIA NIH HHS/United States
- R01 DC013270/DC/NIDCD NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- R01 AG032306/AG/NIA NIH HHS/United States
- R01 NS050915/NS/NINDS NIH HHS/United States
- U54 NS092089/NS/NINDS NIH HHS/United States
- R01 AG045611/AG/NIA NIH HHS/United States
- K24 DC015544/DC/NIDCD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
