

Wisteria floribunda Agglutinin and Its Reactive-Glycan-Carrying Prostate-Specific Antigen as a Novel Diagnostic and Prognostic Marker of Prostate Cancer
- PMID: 28134773
- PMCID: PMC5343797
- DOI: 10.3390/ijms18020261
Wisteria floribunda Agglutinin and Its Reactive-Glycan-Carrying Prostate-Specific Antigen as a Novel Diagnostic and Prognostic Marker of Prostate Cancer
Abstract
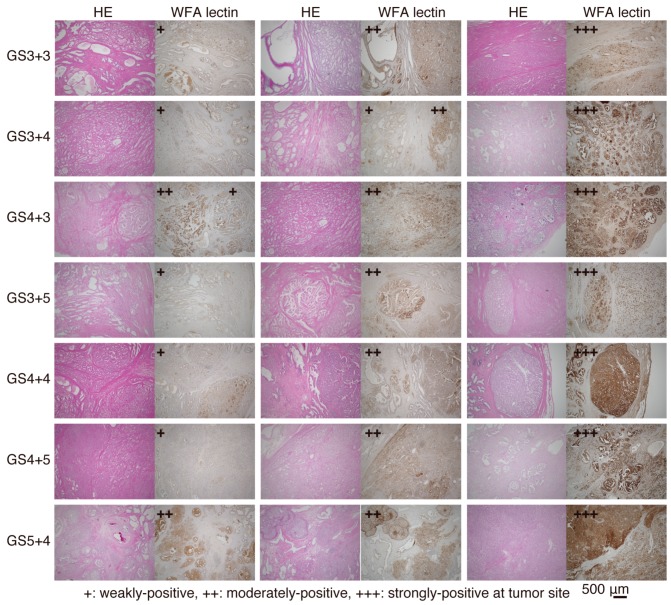
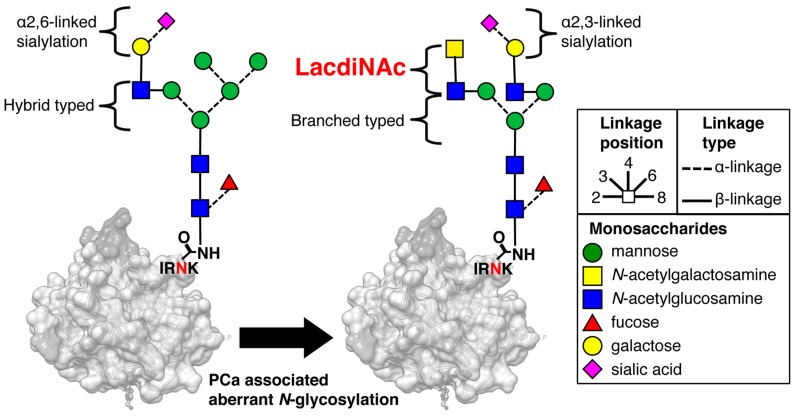
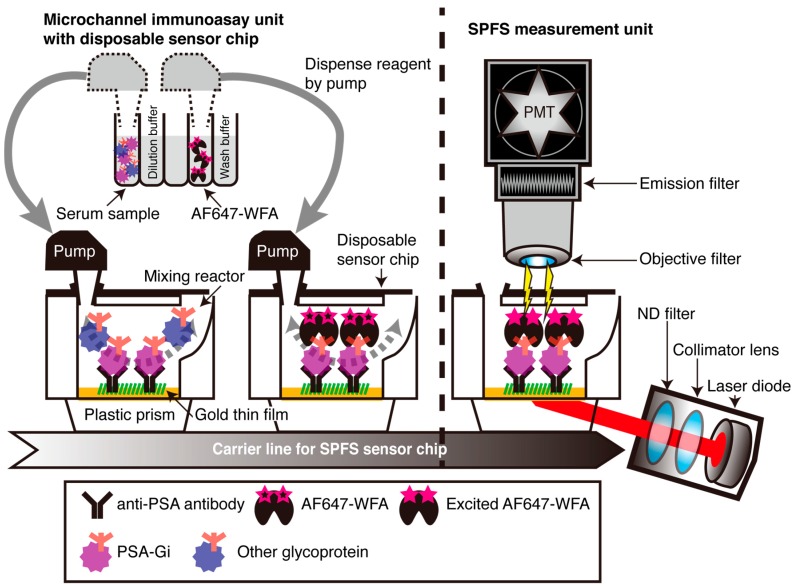
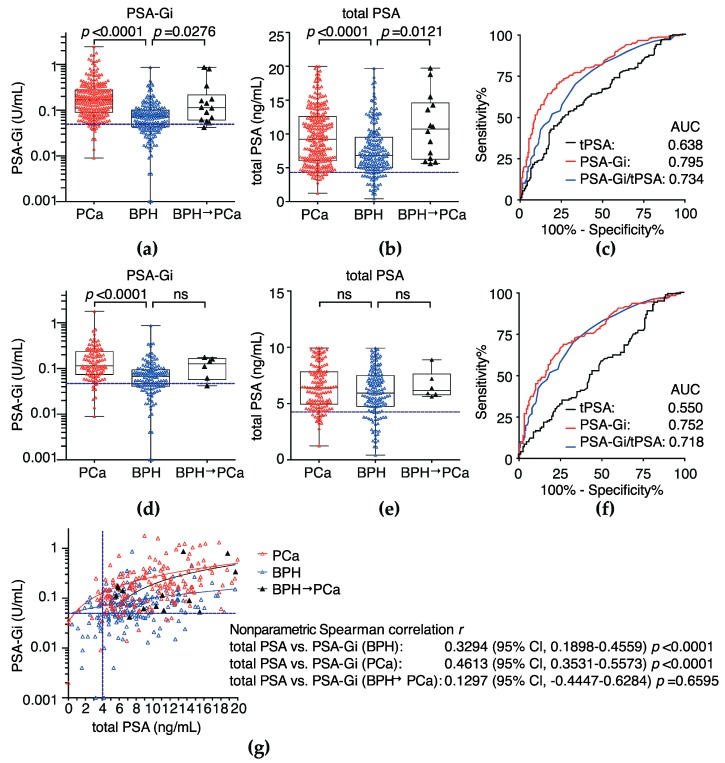
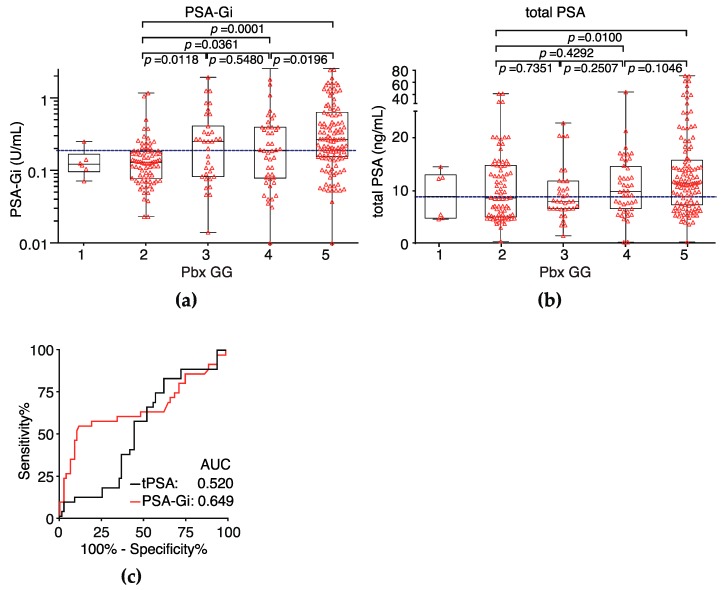
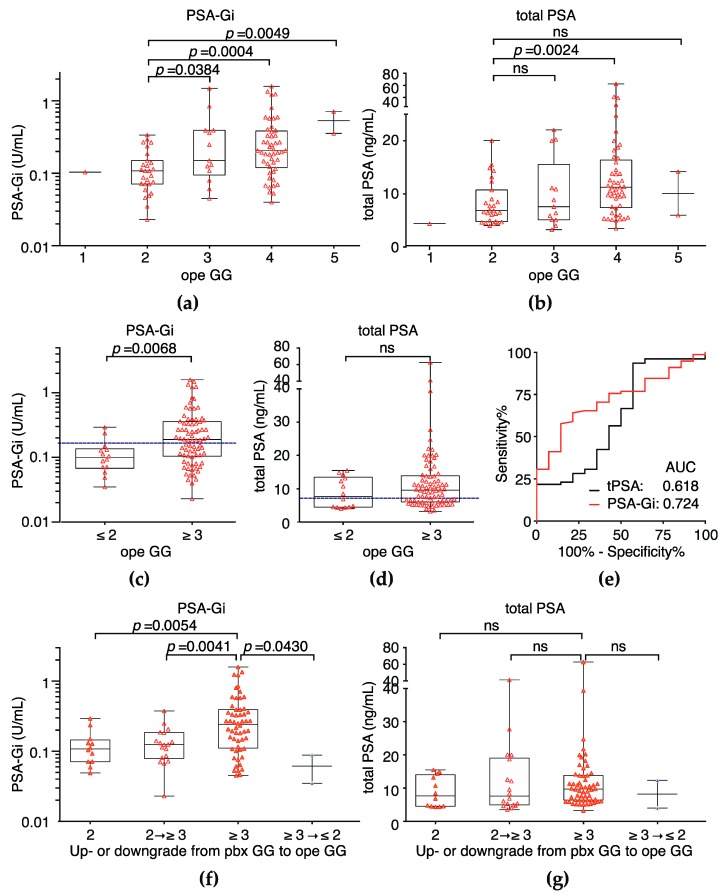
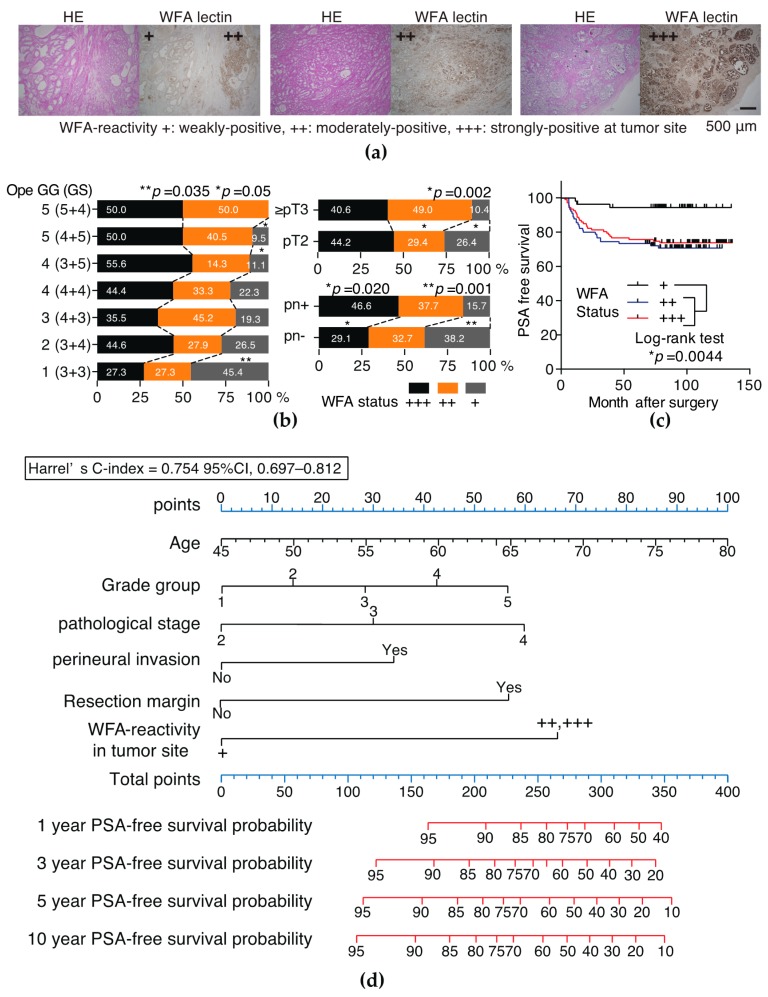
Wisteria floribunda agglutinin (WFA) preferably binds to LacdiNAc glycans, and its reactivity is associated with tumor progression. The aim of this study to examine whether the serum LacdiNAc carrying prostate-specific antigen-glycosylation isomer (PSA-Gi) and WFA-reactivity of tumor tissue can be applied as a diagnostic and prognostic marker of prostate cancer (PCa). Between 2007 and 2016, serum PSA-Gi levels before prostate biopsy (Pbx) were measured in 184 biopsy-proven benign prostatic hyperplasia patients and 244 PCa patients using an automated lectin-antibody immunoassay. WFA-reactivity on tumor was analyzed in 260 radical prostatectomy (RP) patients. Diagnostic and prognostic performance of serum PSA-Gi was evaluated using area under the receiver-operator characteristic curve (AUC). Prognostic performance of WFA-reactivity on tumor was evaluated via Cox proportional hazards regression analysis and nomogram. The AUC of serum PSA-Gi detecting PCa and predicting Pbx Grade Group (GG) 3 and GG ≥ 3 after RP was much higher than those of conventional PSA. Multivariate analysis showed that WFA-reactivity on prostate tumor was an independent risk factor of PSA recurrence. The nomogram was a strong model for predicting PSA-free survival provability with a c-index ≥0.7. Serum PSA-Gi levels and WFA-reactivity on prostate tumor may be a novel diagnostic and pre- and post-operative prognostic biomarkers of PCa, respectively.
Keywords: LacdiNAc; N-glycan; Wisteria floribunda agglutinin (WFA) lectin; biomarker; prostate-specific antigen.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
LacdiNAc-Glycosylated Prostate-specific Antigen Density is a Potential Biomarker of Prostate Cancer.Clin Genitourin Cancer. 2020 Feb;18(1):e28-e36. doi: 10.1016/j.clgc.2019.10.011. Epub 2019 Oct 17. Clin Genitourin Cancer. 2020. PMID: 31711843
-
An Automated Micro-Total Immunoassay System for Measuring Cancer-Associated α2,3-linked Sialyl N-Glycan-Carrying Prostate-Specific Antigen May Improve the Accuracy of Prostate Cancer Diagnosis.Int J Mol Sci. 2017 Feb 22;18(2):470. doi: 10.3390/ijms18020470. Int J Mol Sci. 2017. PMID: 28241428 Free PMC article.
-
A novel glycobiomarker, Wisteria floribunda agglutinin macrophage colony-stimulating factor receptor, for predicting carcinogenesis of liver cirrhosis.Int J Cancer. 2016 Mar 15;138(6):1462-71. doi: 10.1002/ijc.29880. Epub 2015 Oct 20. Int J Cancer. 2016. PMID: 26437001
-
Wisteria floribunda agglutinin positive glycobiomarkers: a unique lectin as a serum biomarker probe in various diseases.Expert Rev Proteomics. 2018 Feb;15(2):183-190. doi: 10.1080/14789450.2018.1419066. Epub 2017 Dec 21. Expert Rev Proteomics. 2018. PMID: 29265940 Review.
-
[Biomarkers of prostate cancer and potential for using ace produced in prostate gland for diagnosis of prostate cancer and benign prostatic hyperplasia].Urologiia. 2019 Jun;(2):73-81. Urologiia. 2019. PMID: 31162906 Review. Russian.
Cited by
-
Highly sensitive biomolecular interaction detection method using optical bound/free separation with grating-coupled surface plasmon field-enhanced fluorescence spectroscopy (GC-SPFS).PLoS One. 2019 Aug 1;14(8):e0220578. doi: 10.1371/journal.pone.0220578. eCollection 2019. PLoS One. 2019. PMID: 31369601 Free PMC article.
-
Clinical significance of the LacdiNAc-glycosylated prostate-specific antigen assay for prostate cancer detection.Cancer Sci. 2019 Aug;110(8):2573-2589. doi: 10.1111/cas.14082. Epub 2019 Jun 27. Cancer Sci. 2019. PMID: 31145522 Free PMC article.
-
Characteristics of α2,3-sialyl N-glycosylated PSA as a biomarker for clinically significant prostate cancer in men with elevated PSA level.Prostate. 2021 Dec;81(16):1411-1427. doi: 10.1002/pros.24239. Epub 2021 Sep 21. Prostate. 2021. PMID: 34549452 Free PMC article.
-
Aberrant N-Glycosylation Profile of Serum Immunoglobulins is a Diagnostic Biomarker of Urothelial Carcinomas.Int J Mol Sci. 2017 Dec 6;18(12):2632. doi: 10.3390/ijms18122632. Int J Mol Sci. 2017. PMID: 29210993 Free PMC article.
-
Glycomics of prostate cancer: updates.Expert Rev Proteomics. 2019 Jan;16(1):65-76. doi: 10.1080/14789450.2019.1549993. Epub 2018 Nov 27. Expert Rev Proteomics. 2019. PMID: 30451032 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
