

Barriers to the Access of Bevacizumab in Patients with Solid Tumors and the Potential Impact of Biosimilars: A Physician Survey
- PMID: 28134851
- PMCID: PMC5374423
- DOI: 10.3390/ph10010019
Barriers to the Access of Bevacizumab in Patients with Solid Tumors and the Potential Impact of Biosimilars: A Physician Survey
Abstract
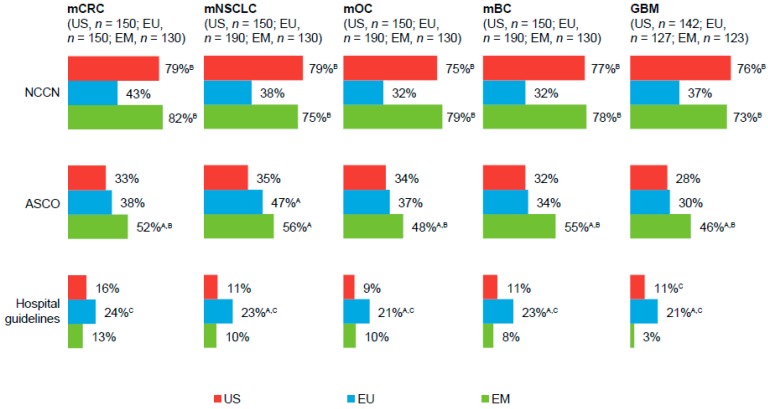
Access to bevacizumab, an important component of oncology treatment regimens, may be limited. This survey of oncologists in the US (n = 150), Europe (n = 230), and emerging markets (EM: Brazil, Mexico, and Turkey; n = 130) examined use of and barriers to accessing bevacizumab as treatment of advanced solid tumors. We also assessed the likelihood that physicians would prescribe a bevacizumab biosimilar, if available. Bevacizumab was frequently used as early-line therapy in metastatic colorectal cancer, metastatic non-squamous non-small-cell lung cancer, and metastatic ovarian cancer (all markets), and as a second-line therapy in glioblastoma multiforme (US, EM). A greater percentage of EM-based physicians cited access-related issues as a barrier to prescribing bevacizumab versus US and EU physicians. Lack of reimbursement and high out-of-pocket costs were cited as predominant barriers to prescribing and common reasons for reducing the number of planned cycles. Overall, ~50% of physicians reported they "definitely" or "probably" would prescribe a bevacizumab biosimilar, if available. Efficacy and safety data in specific tumor types and lower cost were factors cited that would increase likelihood to prescribe a bevacizumab biosimilar. A lower cost bevacizumab biosimilar could address the unmet needs of patients and physicians worldwide, and may have the greatest impact on patient outcomes in EM.
Keywords: access to health care; bevacizumab; biosimilars; colorectal cancer; non–small-cell lung cancer; ovarian cancer.
Conflict of interest statement
Bradley Monk has received honoraria for speakers’ bureau from and has been a consultant for Roche/Genentech; his institution has received research funding from Genentech. Philip Lammers has received compensation for serving on advisory boards with Pfizer Inc. Thomas Cartwright has received compensation for serving as a consultant to and on advisory boards with Bayer, BTG, Genentech, Incyte, Lilly, and Taiho; honoraria from Amgen, AstraZeneca, Celgene, Inccyte, Janssen, and Taiho; and his institution has received research funding from Bayer. Ira Jacobs is a full-time employee of and declares stock holdings and/or stock options from Pfizer Inc.
Figures



Similar articles
-
Bevacizumab in Colorectal Cancer: Current Role in Treatment and the Potential of Biosimilars.Target Oncol. 2017 Oct;12(5):599-610. doi: 10.1007/s11523-017-0518-1. Target Oncol. 2017. PMID: 28801849 Free PMC article. Review.
-
Barriers to the Use of Trastuzumab for HER2+ Breast Cancer and the Potential Impact of Biosimilars: A Physician Survey in the United States and Emerging Markets.Pharmaceuticals (Basel). 2014 Sep 17;7(9):943-53. doi: 10.3390/ph7090943. Pharmaceuticals (Basel). 2014. PMID: 25232798 Free PMC article.
-
Barriers to the Access and Use of Rituximab in Patients with Non-Hodgkin's Lymphoma and Chronic Lymphocytic Leukemia: A Physician Survey.Pharmaceuticals (Basel). 2014 May 7;7(5):530-44. doi: 10.3390/ph7050530. Pharmaceuticals (Basel). 2014. PMID: 24810947 Free PMC article.
-
Clinical and Regulatory Considerations for the Use of Bevacizumab Biosimilars in Metastatic Colorectal Cancer.Clin Colorectal Cancer. 2021 Mar;20(1):42-51.e3. doi: 10.1016/j.clcc.2020.10.005. Epub 2020 Nov 1. Clin Colorectal Cancer. 2021. PMID: 33243618 Review.
-
Biosimilar Use in Breast Cancer Treatment: A National Survey of Brazilian Oncologists' Opinions, Practices, and Concerns.JCO Glob Oncol. 2021 Aug;7:1316-1324. doi: 10.1200/GO.20.00649. JCO Glob Oncol. 2021. PMID: 34415791 Free PMC article.
Cited by
-
PF-06439535 (a Bevacizumab Biosimilar) Compared with Reference Bevacizumab (Avastin®), Both Plus Paclitaxel and Carboplatin, as First-Line Treatment for Advanced Non-Squamous Non-Small-Cell Lung Cancer: A Randomized, Double-Blind Study.BioDrugs. 2019 Oct;33(5):555-570. doi: 10.1007/s40259-019-00363-4. BioDrugs. 2019. PMID: 31338773 Free PMC article. Clinical Trial.
-
Bevacizumab biosimilar LY01008 compared with bevacizumab (Avastin) as first-line treatment for Chinese patients with unresectable, metastatic, or recurrent non-squamous non-small-cell lung cancer: A multicenter, randomized, double-blinded, phase III trial.Cancer Commun (Lond). 2021 Sep;41(9):889-903. doi: 10.1002/cac2.12179. Epub 2021 Jun 29. Cancer Commun (Lond). 2021. PMID: 34184418 Free PMC article. Clinical Trial.
-
Comparison of Efficacy and Safety of a Bevacizumab Biosimilar, in Combination with Chemotherapies, in Nonresectable Metastatic Colorectal Cancer and in Advanced Nonsquamous Non-Small Cell Lung Cancer: A Randomized, Double-Blind, Phase III Study.South Asian J Cancer. 2023 Oct 13;13(1):66-76. doi: 10.1055/s-0043-1774403. eCollection 2024 Jan. South Asian J Cancer. 2023. PMID: 38721097 Free PMC article.
-
Safety and efficacy of bevacizumab biosimilar in recurrent/ progressive glioblastoma.Ecancermedicalscience. 2021 Jan 13;15:1166. doi: 10.3332/ecancer.2021.1166. eCollection 2021. Ecancermedicalscience. 2021. PMID: 33680080 Free PMC article.
-
The Impact of Palliative Chemotherapy on the Survival of Patients With Metastatic Colorectal Cancer in Jordan.Cureus. 2023 Sep 29;15(9):e46187. doi: 10.7759/cureus.46187. eCollection 2023 Sep. Cureus. 2023. PMID: 37790030 Free PMC article.
References
-
- Avastin® (Bevacizumab) US Prescribing Information. [(accessed on22 February 2016)]. Available online: http://www.gene.com/download/pdf/avastin_prescribing.pdf.
-
- Presta L.G., Chen H., O’Connor S.J., Chisholm V., Meng Y.G., Krummen L., Winkler M., Ferrara N. Humanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disorders. Cancer Res. 1997;57:4593–4599. - PubMed
-
- Summary of Product Characteristics: Avastin (Bevacizumab) [(accessed on22 February 2016)]. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_....
-
- Ferrara N. Role of vascular endothelial growth factor in regulation of physiological angiogenesis. Am. J. Physiol. Cell Physiol. 2001;280:C1358–C1366. - PubMed
-
- Fox W.D., Higgins B., Maiese K.M., Drobnjak M., Cordon-Cardo C., Scher H.I., Agus D.B. Antibody to vascular endothelial growth factor slows growth of an androgen-independent xenograft model of prostate cancer. Clin. Cancer Res. 2002;8:3226–3231. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
