TAFRO syndrome: New subtype of idiopathic multicentric Castleman disease
- PMID: 28135567
- PMCID: PMC5474112
- DOI: 10.17305/bjbms.2017.1930
TAFRO syndrome: New subtype of idiopathic multicentric Castleman disease
Abstract
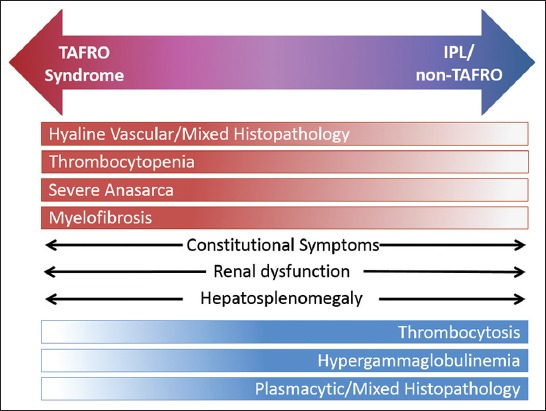
Castleman disease (CD) describes a group of three rare and poorly understood lymphoproliferative disorders that have heterogeneous clinical symptoms and common lymph node histopathological features. Unicentric CD (UCD) involves a single region of enlarged nodes. Multicentric CD (MCD) involves multiple regions of enlarged lymph nodes, constitutional symptoms, and organ dysfunction due to a cytokine storm often including interleukin 6. MCD is further divided into Human Herpes Virus-8 (HHV-8)-associated MCD, which occurs in immunocompromised individuals, and HHV-8-negative/idiopathic MCD (iMCD). Recently, iMCD has been further sub-divided into patients with TAFRO syndrome, which involves thrombocytopenia (T), anasarca (A), fevers (F), reticulin myelofibrosis (R), organomegaly (O), and normal or only slightly elevated immunoglobulin levels, and those who do not have TAFRO syndrome. Non-TAFRO iMCD patients typically have thrombocytosis, less severe fluid accumulation, and hypergammaglobulinemia. iMCD patients with TAFRO syndrome may have a worse prognosis, but more research is needed.
Figures
References
-
- Castleman B, Towne VW. Case records of the Massachusetts General Hospital: Case No. 40231. N Engl J Med. 1954;250(23):1001–5. https://doi.org/10.1056/NEJM195406102502308. - PubMed
-
- Castleman B, Iverson L, Menendez VP. Localized mediastinal lymph node hyperplasia resembling thymoma. Cancer. 1956;9(4):822–30. https://doi.org/10.1002/1097-0142(195607/08)9: 4<822: AID-CNCR2820090430>3.0.CO;2-4. - PubMed
-
- Gaba AR, Stein RS, Sweet DL, Varikojis D. Multicentric giant lymph node hyperplasia. Am J Clin Pathol. 1978;69(1):86–90. https://doi.org/10.1093/ajcp/69.1.86. - PubMed
-
- Bowne WB, Lewis JJ, Filippa DA, Niesvizky R, Brooks AD, Burt ME, et al. The management of unicentric and multicentric Castleman’s disease: A report of 16 cases and a review of the literature. Cancer. 1999;85(3):706–17. https://doi.org/10.1002/(SICI)1097-0142(19990201)85: 3<706: AID-CNCR21>3.0.CO;2-7. - PubMed
-
- Waterston A, Bower M. Fifty years of multicentric Castleman’s disease. Acta Oncol. 2004;43(8):698–704. https://doi.org/10.1080/02841860410002752. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources