

A Randomized Controlled Trial of Ethyl Glucuronide-Based Contingency Management for Outpatients With Co-Occurring Alcohol Use Disorders and Serious Mental Illness
- PMID: 28135843
- PMCID: PMC5378651
- DOI: 10.1176/appi.ajp.2016.16050627
A Randomized Controlled Trial of Ethyl Glucuronide-Based Contingency Management for Outpatients With Co-Occurring Alcohol Use Disorders and Serious Mental Illness
Erratum in
-
CORRECTIONS.Am J Psychiatry. 2017 Jun 1;174(6):604. doi: 10.1176/appi.ajp.2017.1746correction1. Am J Psychiatry. 2017. PMID: 28565953 No abstract available.
Abstract
Objective: The authors examined whether a contingency management intervention using the ethyl glucuronide (EtG) alcohol biomarker resulted in increased alcohol abstinence in outpatients with co-occurring serious mental illnesses. Secondary objectives were to determine whether contingency management was associated with changes in heavy drinking, treatment attendance, drug use, cigarette smoking, psychiatric symptoms, and HIV-risk behavior.
Method: Seventy-nine (37% female, 44% nonwhite) outpatients with serious mental illness and alcohol dependence receiving treatment as usual completed a 4-week observation period and were randomly assigned to 12 weeks of contingency management for EtG-negative urine samples and addiction treatment attendance, or reinforcement only for study participation. Contingency management included the variable magnitude of reinforcement "prize draw" procedure contingent on EtG-negative samples (<150 ng/mL) three times a week and weekly gift cards for outpatient treatment attendance. Urine EtG, drug test, and self-report outcomes were assessed during the 12-week intervention and 3-month follow-up periods.
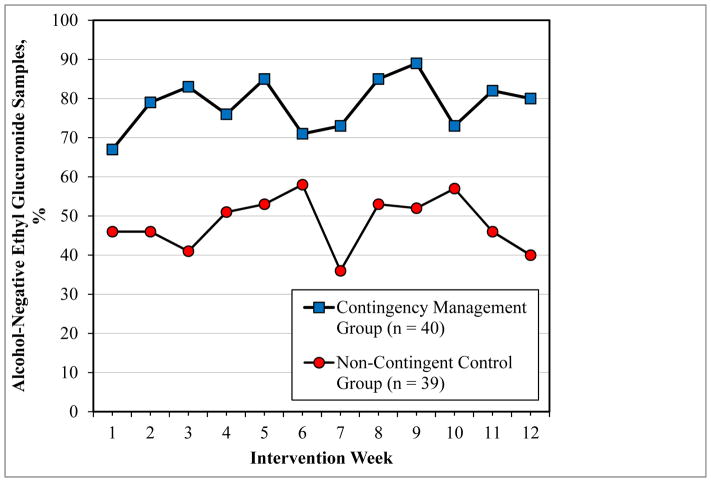
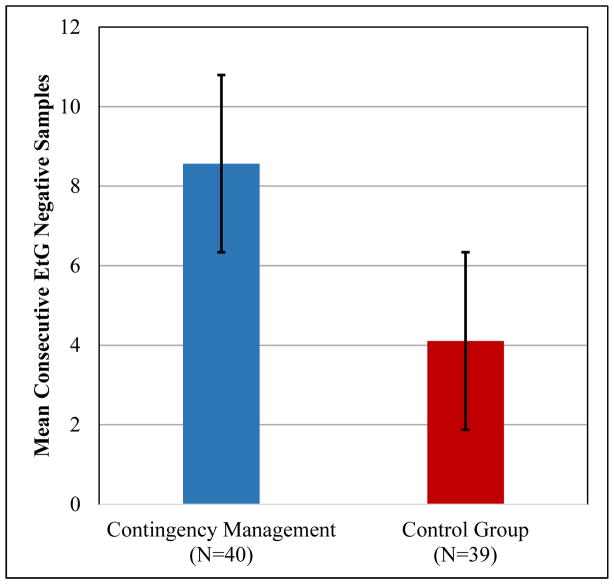
Results: Contingency management participants were 3.1 times (95% CI=2.2-4.5) more likely to submit an EtG-negative urine test during the 12-week intervention period, attaining nearly 1.5 weeks of additional alcohol abstinence compared with controls. Contingency management participants had significantly lower mean EtG levels, reported less drinking and fewer heavy drinking episodes, and were more likely to submit stimulant-negative urine and smoking-negative breath samples, compared with controls. Differences in self-reported alcohol use were maintained at the 3-month follow-up.
Conclusions: This is the first randomized trial utilizing an accurate and validated biomarker (EtG) to demonstrate the efficacy of contingency management for alcohol dependence in outpatients with serious mental illness.
Keywords: Alcohol Abuse; Biological Markers; Chronic Psychiatric Illness.
Figures
Comment in
-
Reducing Alcohol Use Via Contingency Management and Verification Using a Urine Biomarker.Am J Psychiatry. 2017 Apr 1;174(4):309-310. doi: 10.1176/appi.ajp.2016.16121375. Am J Psychiatry. 2017. PMID: 28366096 No abstract available.
References
-
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291:1238–1245. - PubMed
-
- Bouchery EE, Harwood HJ, Sacks JJ, Simon CJ, Brewer RD. Economic costs of excessive alcohol consumption in the U.S., 2006. Am J Prev Med. 2011;41:516–524. - PubMed
-
- Cohen E, Feinn R, Arias A, Kranzler HR. Alcohol treatment utilization: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2007;86:214–221. - PubMed
-
- Buckley PF. Prevalence and consequences of the dual diagnosis of substance abuse and severe mental illness. J Clin Psychiatry. 2006;67(Suppl 7):5–9. - PubMed
-
- Lohr JB, Flynn K. Smoking and schizophrenia. Schizophr Res. 1992;8:93–102. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
