

Outcome of Large Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features
- PMID: 28136139
- PMCID: PMC5385447
- DOI: 10.1089/thy.2016.0649
Outcome of Large Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features
Abstract
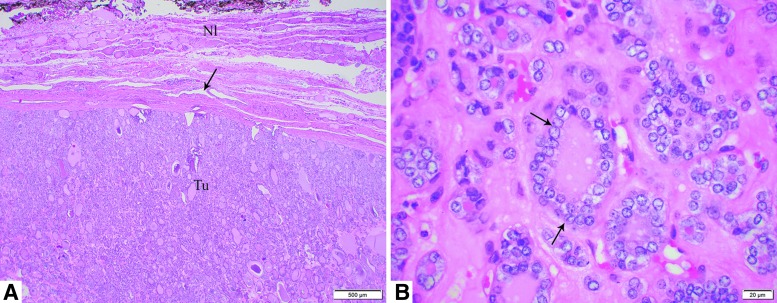
Background: In 2016, encapsulated follicular variant of papillary thyroid carcinoma without invasion was renamed "noninvasive follicular thyroid neoplasm with papillary-like nuclear features" (NIFTP) in order to reduce overtreatment of this indolent tumor. However, many endocrinologists remain uneasy about managing large (≥4 cm) NIFTP conservatively without radioactive iodine (RAI) therapy. The objectives of this study are to characterize the clinicopathologic characteristics and outcome of large NIFTP in order to assist therapeutic decision making.
Methods: The pathology databases of four tertiary hospitals were searched for large (≥4 cm) NIFTP. Cases with separate foci of carcinoma were excluded. Seventy-nine cases fulfilled the inclusion criteria. Among them, 56 (71%) had at least two years of clinical follow-up (FU), and 49 (62%) had four or more years of FU. The clinicopathologic characteristics were reviewed and documented by four endocrine pathologists.
Results: The median size of the NIFTP was 4.5 cm (range 4.0-8.0 cm). The entire capsule was sampled in 50 (63%) tumors, while in the remaining 29 (37%) cases, it was submitted representatively, with a median of 2.1 blocks per centimeter of tumor examined. Large NIFTP had a female preponderance with a male:female ratio of 1:1.8, and presented at a median age of 49 years. There were no lymph node metastases at diagnosis in any of the patients, and none of the patients (n = 25) in whom nodal tissue was available for microscopic examination had positive findings. Twenty-six (33%) underwent thyroid lobectomy alone, and 37 (47%) did not receive RAI ablation. No recurrence was observed in the entire cohort, including all 32 patients with two or more years of FU who did not receive RAI therapy (median FU: 6.7 years). Among patients with four or more years of FU, all 25 individuals without RAI therapy did not recur, with a median FU of 11.2 years. Patients with a larger tumor size tended to receive postoperative RAI ablation (p = 0.001).
Conclusions: Similar to their small counterparts, large NIFTP appear to have an extremely low risk of recurrence (zero in this cohort), even when treated conservatively without RAI therapy. Surgical treatment alone, including lobectomy, appears to be adequate for large NIFTP.
Keywords: follicular variant; noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP); papillary thyroid carcinoma; radioactive iodine.
Conflict of interest statement
No competing financial interests exist for all contributory authors.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. 2014. Cancer statistics, 2014. CA Cancer J Clin 64:9–29 - PubMed
-
- Jung CK, Little MP, Lubin JH, Brenner AV, Wells SA, Jr, Sigurdson AJ, Nikiforov YE. 2014. The increase in thyroid cancer incidence during the last four decades is accompanied by a high frequency of BRAF mutations and a sharp increase in RAS mutations. J Clin Endocrinol Metab 99:E276–285 - PMC - PubMed
-
- Nikiforov YE, Seethala RR, Tallini G, Baloch ZW, Basolo F, Thompson LD, Barletta JA, Wenig BM, Al Ghuzlan A, Kakudo K, Giordano TJ, Alves VA, Khanafshar E, Asa SL, El-Naggar AK, Gooding WE, Hodak SP, Lloyd RV, Maytal G, Mete O, Nikiforova MN, Nose V, Papotti M, Poller DN, Sadow PM, Tischler AS, Tuttle RM, Wall KB, LiVolsi VA, Randolph GW, Ghossein RA. 2016. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol 2:1023–1029 - PMC - PubMed
-
- DeLellis RA, Lloyd RV, Heitz PU, Eng C. 2004. Pathology and Genetics of Tumours of the Endocrine Organs. IARC Press, Lyon, France
-
- Agrawal N, Akbani R, Aksoy BA, Ally A, Arachchi H, Asa SL, Auman JT, Balasundaram M, Balu S, Baylin SB, Behera M, Bernard B, Beroukhim R, Bishop JA, Black AD, Bodenheimer T, Boice L, Bootwalla MS, Bowen J, Bowlby R, Bristow CA, Brookens R, Brooks D, Bryant R, Buda E, Butterfield YSN, Carling T, Carlsen R, Carter SL, Carty SE, Chan TA, Chen AY, Cherniack AD, Cheung D, Chin L, Cho J, Chu A, Chuah E, Cibulskis K, Ciriello G, Clarke A, Clayman GL, Cope L, Copland J, Covington K, Danilova L, Davidsen T, Demchok JA, DiCara D, Dhalla N, Dhir R, Dookran SS, Dresdner G, Eldridge J, Eley G, El-Naggar AK, Eng S, Fagin JA, Fennell T, Ferris RL, Fisher S, Frazer S, Frick J, Gabriel SB, Ganly I, Gao J, Garraway LA, Gastier-Foster JM, Getz G, Gehlenborg N, Ghossein R, Gibbs RA, Giordano TJ, Gomez-Hernandez K, Grimsby J, Gross B, Guin R, Hadjipanayis A, Harper HA, Hayes DN, Heiman DI, Herman JG, Hoadley KA, Hofree M, Holt RA, Hoyle AP, Huang SW, Huang M, Hutter CM, Ideker T, Iype L, Jacobsen A, Jefferys SR, Jones CD, Jones SJM, Kasaian K, Kebebew E, Khuri FR, Kim J, Kramer R, Kreisberg R, Kucherlapati R, Kwiatkowski DJ, Ladanyi M, Lai PH, Laird PW, Lander E, Lawrence MS, Lee D, Lee E, Lee S, Lee W, Leraas KM, Lichtenberg TM, Lichtenstein L, Lin P, Ling S, Liu J, Liu W, Liu Y, LiVolsi VA, Lu Y, Ma Y, Mahadeshwar HS, Marra MA, Mayo M, McFadden DG, Meng S, Meyerson M, Mieczkowski PA, Miller M, Mills G, Moore RA, Mose LE, Mungall AJ, Murray BA, Nikiforov YE, Noble MS, Ojesina AI, Owonikoko TK, Ozenberger BA, Pantazi A, Parfenov M, Park PJ, Parker JS, Paull EO, Pedamallu CS, Perou CM, Prins JF, Protopopov A, Ramalingam SS, Ramirez NC, Ramirez R, Raphael BJ, Rathmell WK, Ren X, Reynolds SM, Rheinbay E, Ringel MD, Rivera M, Roach J, Robertson AG, Rosenberg MW, Rosenthall M, Sadeghi S, Saksena G, Sander C, Santoso N, Schein JE, Schultz N, Schumacher SE, Seethala RR, Seidman J, Senbabaoglu Y, Seth S, Sharpe S, Mills Shaw KR, Shen JP, Shen R, Sherman S, Sheth M, Shi Y, Shmulevich I, Sica GL, Simons JV, Sipahimalani P, Smallridge RC, Sofia HJ, Soloway MG, Song X, Sougnez C, Stewart C, Stojanov P, Stuart JM, Tabak B, Tam A, Tan D, Tang J, Tarnuzzer R, Taylor BS, Thiessen N, Thorne L, Thorsson V, Tuttle RM, Umbricht CB, Van Den Berg DJ, Vandin F, Veluvolu U, Verhaak RGW, Vinco M, Voet D, Walter V, Wang Z, Waring S, Weinberger PM, Weinstein JN, Weisenberger DJ, Wheeler D, Wilkerson MD, Wilson J, Williams M, Winer DA, Wise L, Wu J, Xi L, Xu AW, Yang L, Yang L, Zack TI, Zeiger MA, Zeng D, Zenklusen JC, Zhao N, Zhang H, Zhang J, Zhang J, Zhang W, Zmuda E, Zou L. 2014. Integrated genomic characterization of papillary thyroid carcinoma. Cell 159:676–690 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
