

Induction of metastasis, cancer stem cell phenotype, and oncogenic metabolism in cancer cells by ionizing radiation
- PMID: 28137309
- PMCID: PMC5282724
- DOI: 10.1186/s12943-016-0577-4
Induction of metastasis, cancer stem cell phenotype, and oncogenic metabolism in cancer cells by ionizing radiation
Abstract
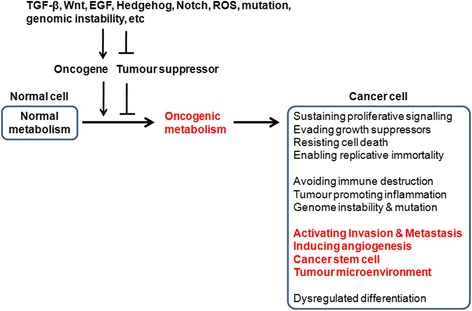
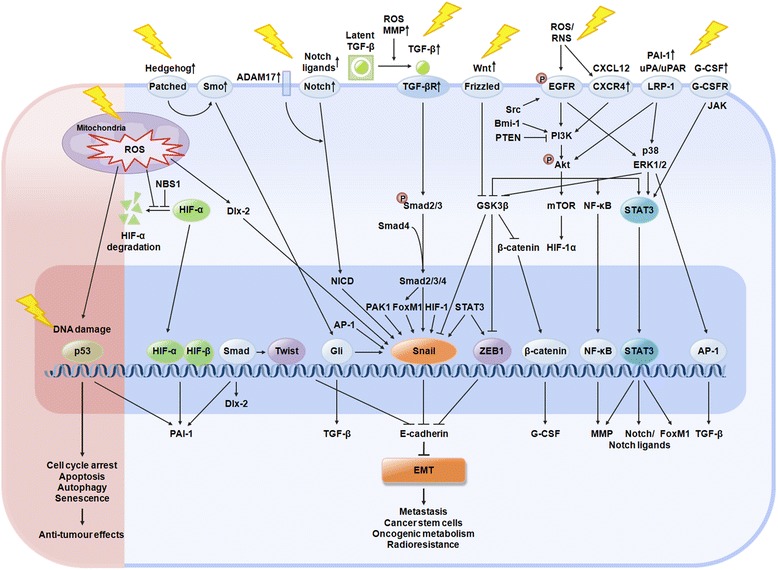
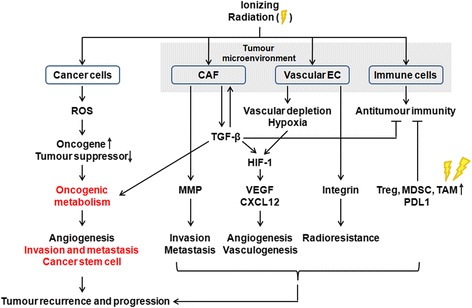
Radiation therapy is one of the major tools of cancer treatment, and is widely used for a variety of malignant tumours. Radiotherapy causes DNA damage directly by ionization or indirectly via the generation of reactive oxygen species (ROS), thereby destroying cancer cells. However, ionizing radiation (IR) paradoxically promotes metastasis and invasion of cancer cells by inducing the epithelial-mesenchymal transition (EMT). Metastasis is a major obstacle to successful cancer therapy, and is closely linked to the rates of morbidity and mortality of many cancers. ROS have been shown to play important roles in mediating the biological effects of IR. ROS have been implicated in IR-induced EMT, via activation of several EMT transcription factors-including Snail, HIF-1, ZEB1, and STAT3-that are activated by signalling pathways, including those of TGF-β, Wnt, Hedgehog, Notch, G-CSF, EGFR/PI3K/Akt, and MAPK. Cancer cells that undergo EMT have been shown to acquire stemness and undergo metabolic changes, although these points are debated. IR is known to induce cancer stem cell (CSC) properties, including dedifferentiation and self-renewal, and to promote oncogenic metabolism by activating these EMT-inducing pathways. Much accumulated evidence has shown that metabolic alterations in cancer cells are closely associated with the EMT and CSC phenotypes; specifically, the IR-induced oncogenic metabolism seems to be required for acquisition of the EMT and CSC phenotypes. IR can also elicit various changes in the tumour microenvironment (TME) that may affect invasion and metastasis. EMT, CSC, and oncogenic metabolism are involved in radioresistance; targeting them may improve the efficacy of radiotherapy, preventing tumour recurrence and metastasis. This study focuses on the molecular mechanisms of IR-induced EMT, CSCs, oncogenic metabolism, and alterations in the TME. We discuss how IR-induced EMT/CSC/oncogenic metabolism may promote resistance to radiotherapy; we also review efforts to develop therapeutic approaches to eliminate these IR-induced adverse effects.
Keywords: Cancer stem cells; Epithelial-mesenchymal transition; Metastasis; Oncogenic metabolism; Radioresistance; Radiotherapy; Reactive oxygen species; Snail; Tumour microenvironment.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
