

Risk factors for gallbladder contractility after cholecystolithotomy in elderly high-risk surgical patients
- PMID: 28138229
- PMCID: PMC5238807
- DOI: 10.2147/CIA.S125139
Risk factors for gallbladder contractility after cholecystolithotomy in elderly high-risk surgical patients
Abstract
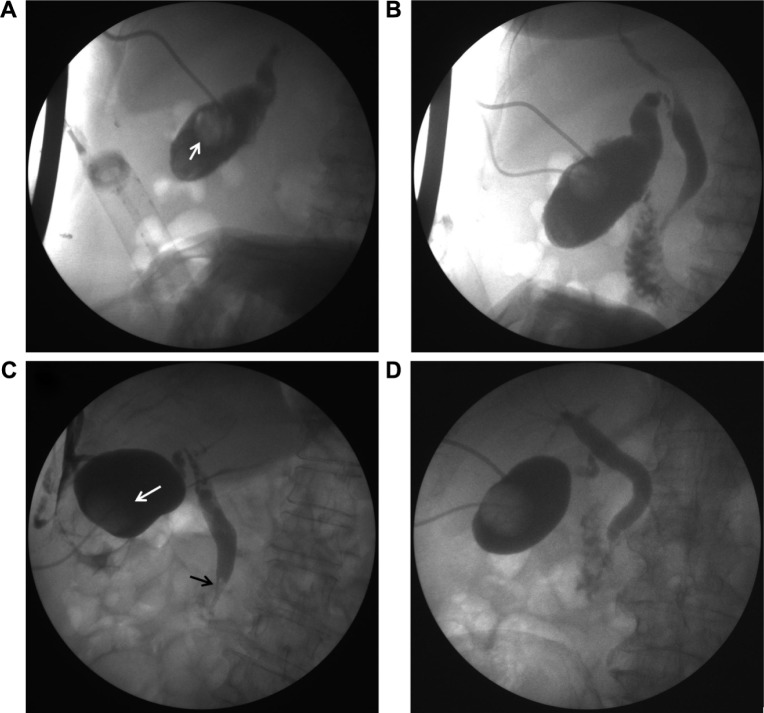
Objective: Cholecystolithiasis is a common disease in the elderly patient. The routine therapy is open or laparoscopic cholecystectomy. In the previous study, we designed a minimally invasive cholecystolithotomy based on percutaneous cholecystostomy combined with a choledochoscope (PCCLC) under local anesthesia.
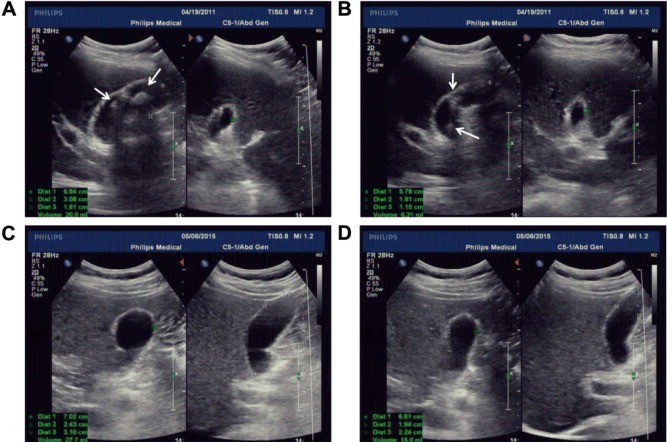
Methods: To investigate the effect of PCCLC on the gallbladder contractility function, PCCLC and laparoscope combined with a choledochoscope were compared in this study.
Results: The preoperational age and American Society of Anesthesiologists (ASA) scores, as well as postoperational lithotrity rate and common biliary duct stone rate in the PCCLC group, were significantly higher than the choledochoscope group. However, the pre- and postoperational gallbladder ejection fraction was not significantly different. Univariable and multivariable logistic regression analyses indicated that the preoperational thickness of gallbladder wall (odds ratio [OR]: 0.540; 95% confidence interval [CI]: 0.317-0.920; P=0.023) and lithotrity (OR: 0.150; 95% CI: 0.023-0.965; P=0.046) were risk factors for postoperational gallbladder ejection fraction. The area under receiver operating characteristics curve was 0.714 (P=0.016; 95% CI: 0.553-0.854).
Conclusion: PCCLC strategy should be carried out cautiously. First, restricted by the diameter of the drainage tube, the PCCLC should be used only for small gallstones in high-risk surgical patients. Second, the usage of lithotrity should be strictly limited to avoid undermining the gallbladder contractility and increasing the risk of secondary common bile duct stones.
Keywords: GBEF; cholecystolithotomy; gallbladder motility; lithotrity; thickness of gallbladder wall.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



Similar articles
-
Ultrasound-guided double-tract percutaneous cholecystostomy combined with a choledochoscope for performing cholecystolithotomies in high-risk surgical patients.Surg Endosc. 2014 Jul;28(7):2236-42. doi: 10.1007/s00464-014-3451-8. Epub 2014 Feb 26. Surg Endosc. 2014. PMID: 24570012
-
Palliative percutaneous transhepatic gallbladder drainage of gallbladder empyema before laparoscopic cholecystectomy.Hepatogastroenterology. 2000 Jul-Aug;47(34):932-6. Hepatogastroenterology. 2000. PMID: 11020851
-
Combined surgical and radiologic intervention for complicated cholelithiasis in high-risk patients.Radiology. 1987 Dec;165(3):715-9. doi: 10.1148/radiology.165.3.3317502. Radiology. 1987. PMID: 3317502
-
Percutaneous biliary interventions through the gallbladder and the cystic duct: What radiologists need to know.Clin Radiol. 2014 Dec;69(12):1304-11. doi: 10.1016/j.crad.2014.07.016. Epub 2014 Aug 27. Clin Radiol. 2014. PMID: 25172204 Review.
-
Cholecystostomy and transcholecystic biliary access.Tech Vasc Interv Radiol. 2008 Mar;11(1):2-13. doi: 10.1053/j.tvir.2008.05.002. Tech Vasc Interv Radiol. 2008. PMID: 18725137 Review.
Cited by
-
Reconsideration of indications for choledochoscopic gallbladder-preserving surgery and preventive measures for postoperative recurrence of gallstones.Wideochir Inne Tech Maloinwazyjne. 2020 Mar;15(1):87-96. doi: 10.5114/wiitm.2019.88647. Epub 2019 Oct 17. Wideochir Inne Tech Maloinwazyjne. 2020. PMID: 32117490 Free PMC article.
References
-
- Tan YY, Zhao G, Wang D, Wang JM, Tang JR, Ji ZL. A new strategy of minimally invasive surgery for cholecystolithiasis: calculi removal and gallbladder preservation. Dig Surg. 2013;30(4–6):466–471. - PubMed
-
- Rabenstein T, Radespiel-Troger M, Hopfner L, et al. Ten years experience with piezoelectric extracorporeal shockwave lithotripsy of gallbladder stones. Eur J Gastroenterol Hepatol. 2005;17(6):629–639. - PubMed
-
- Tazuma S, Nishioka T, Ochi H, et al. Impaired gallbladder mucosal function in aged gallstone patients suppresses gallstone recurrence after successful extracorporeal shockwave lithotripsy. J Gastroenterol Hepatol. 2003;18(2):157–161. - PubMed
-
- Wang T, Chen T, Zou S, et al. Ultrasound-guided double-tract percutaneous cholecystostomy combined with a choledochoscope for performing cholecystolithotomies in high-risk surgical patients. Surg Endosc. 2014;28(7):2236–2242. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
