

The impact of changes in intensive care organization on patient outcome and cost-effectiveness-a narrative review
- PMID: 28138389
- PMCID: PMC5264296
- DOI: 10.1186/s40560-016-0207-7
The impact of changes in intensive care organization on patient outcome and cost-effectiveness-a narrative review
Abstract
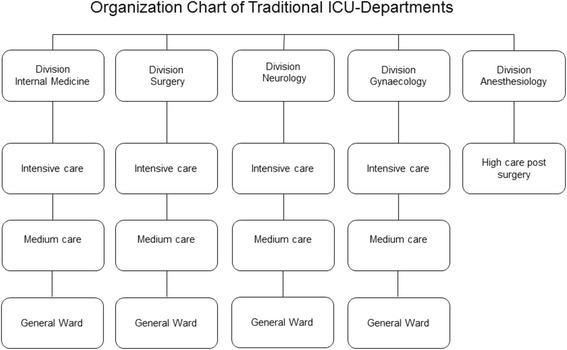
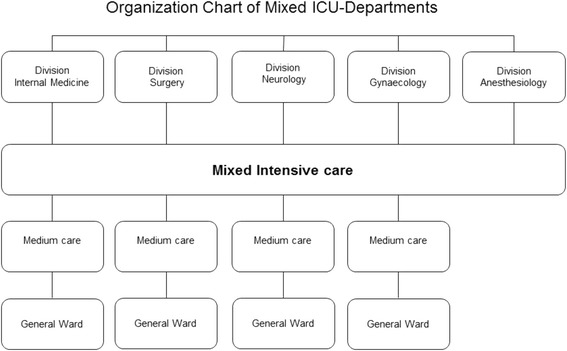
The mortality rate of critically ill patients is high and the cost of the intensive (ICU) department is among the highest within the health-care industry. The cost will continue to increase because of the aging population in the western world. In the present review, we will discuss the impact of changes in ICU department organization on patient outcome and cost-effectiveness. The general perception that drug and treatment discoveries are the main drivers behind improved patient outcome within the health-care industry is in general not true. This is especially the case for the ICU department, in which the past decades' organizational changes were the main drivers behind the reduction of ICU mortality. These interventions were at the same time able to reduce cost, something which is rare for drug and treatment discoveries. The organization of the intensive care department has been changed over the past decades, resulting in better patient outcome and reduction of cost. Major changes are the implementation of the "closed format" and electronic patient record. Furthermore, we will present possible future options to improve the organization of the ICU department to further reduce mortality and cost such as pooling of dedicated ICU into mixed ICU and embedding business strategies such as lean and total quality management. Challenges are ahead as the ICU is taking up the largest share of national health-care expenditure, and with the aging of the population, this will continue to increase. Besides future improvements of organizational structures within the ICU, the focus should also be on the implementation of and compliance with proven beneficial organizational structures.
Keywords: Closed and open format; Critically ill; Intensive care department; Lean; Management; Organization; Pooling; Six Sigma; Total quality management.
Figures
References
-
- Carson SS, Stocking C, Podsadecki T, Christenson J, Pohlman A, MacRae S, Jordan J, Humphrey H, Siegler M, Hall J. Effects of organizational change in the medical intensive care unit of a teaching hospital: a comparison of 'open' and 'closed' formats. Jama. 1996;276:322–328. doi: 10.1001/jama.1996.03540040066035. - DOI - PubMed
-
- Multz AS, Chalfin DB, Samson IM, Dantzker DR, Fein AM, Steinberg HN, Niederman MS, Scharf SM. A "closed" medical intensive care unit (MICU) improves resource utilization when compared with an "open" MICU. Am J Respir Crit Care Med. 1998;157:1468–1473. doi: 10.1164/ajrccm.157.5.9708039. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
