

Hybrid surgery for early gastric cancer
- PMID: 28138593
- PMCID: PMC5244614
- DOI: 10.21037/tgh.2016.03.23
Hybrid surgery for early gastric cancer
Abstract
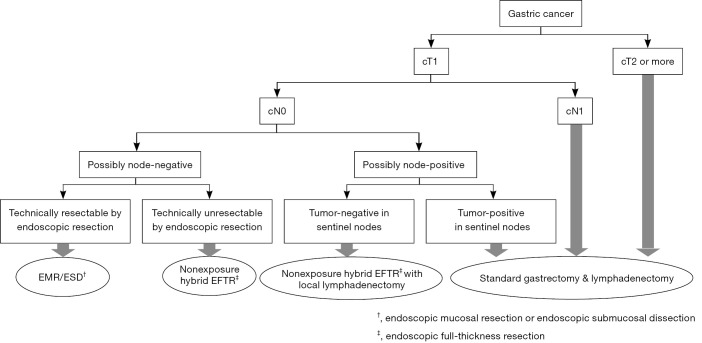
Endoscopic submucosal dissection (ESD) is the most suitable treatment option in terms of minimally invasive treatment for potential node-negative early gastric cancers (EGCs). Furthermore, making the resection area of the primary lesion as small as possible is ideal for the patient's quality of life, even for potential node-positive EGC. An endoluminal approach is a reasonable option with which to minimize stomach resection area, because this procedure can be accurately demarcated from the inside. From this point of view, endoscopic full-thickness resection (EFTR) may be optimal, while laparoscopic assistance would be more desirable to create a more secure procedure. However, hybrid EFTR for EGCs has two limitations, which must be solved. First, concerns regarding iatrogenic tumor seeding via transluminal communication between the inside and outside of the tract exist. The second limitation relates to the determination of lymphadenectomy. Conventional lymphadenectomy, which involves the removal of the majority of feeding arteries, can lead to necrosis of the remaining gastric wall. Therefore, the resection area of lymphadenectomy should also be carefully determined. To address these two problems, a non-exposed hybrid EFTR combined with sentinel node navigation surgery (SNNS) would be the most ideal method of minimally invasive surgery for EGCs.
Keywords: Minimally invasive gastrectomy; endoscopic full-thickness resection (EFTR); hybrid surgery; non-exposure method; sentinel node navigation surgery (SNNS).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Yahagi N, Uraoka T, Ida Y, et al. Endoscopic submucosal dissection using the flex and the dual knives. Techn Gastrointest Endosc 2011;13:74-8. 10.1016/j.tgie.2011.02.006 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous