

The intensive care medicine agenda on acute kidney injury
- PMID: 28138736
- PMCID: PMC5534380
- DOI: 10.1007/s00134-017-4687-2
The intensive care medicine agenda on acute kidney injury
Abstract
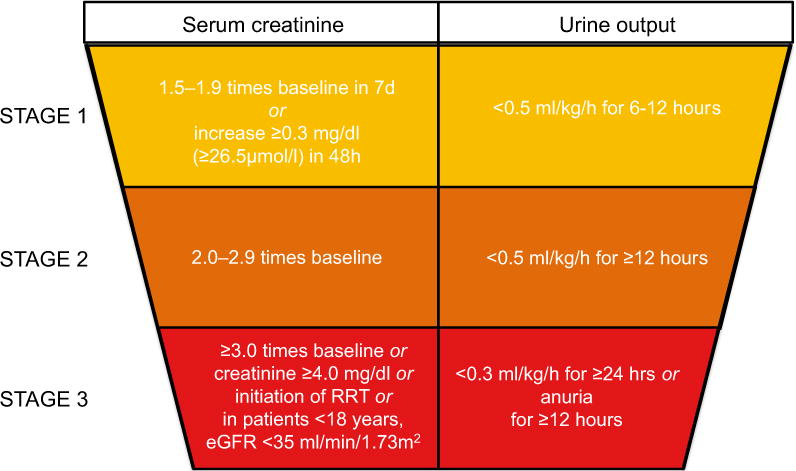
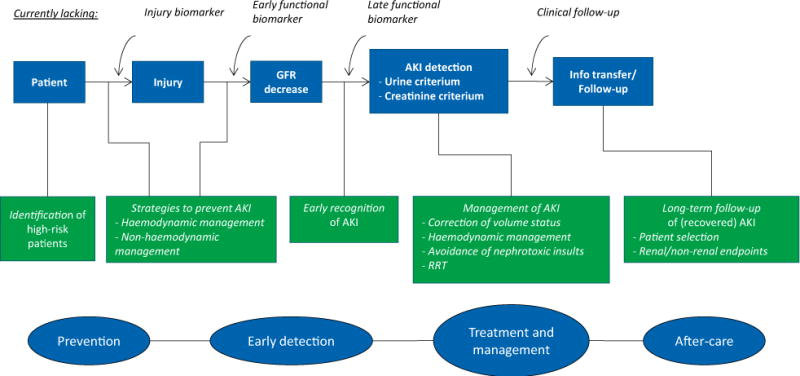
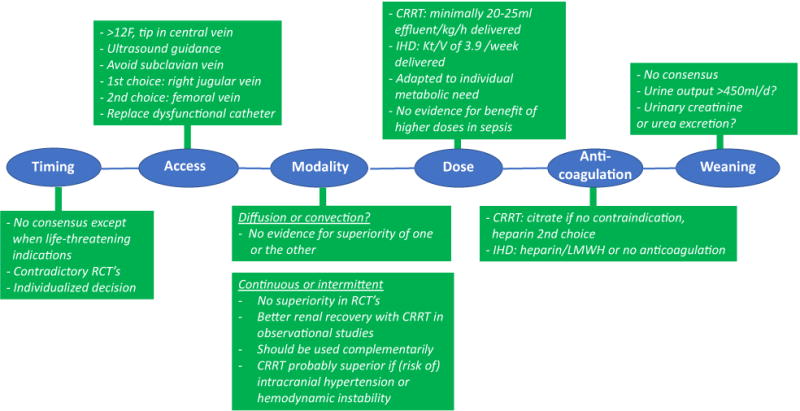
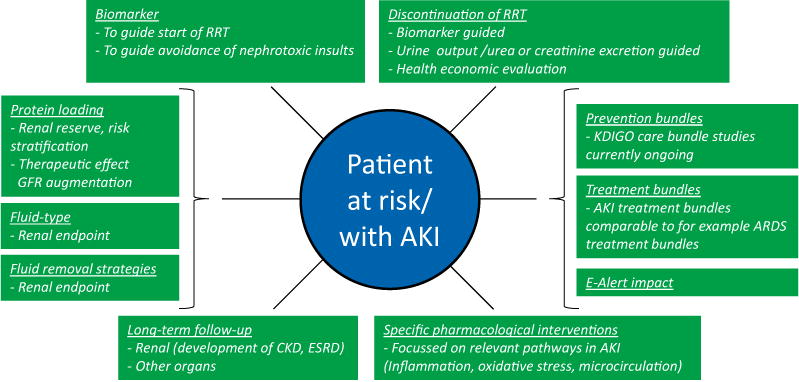
Acute kidney injury (AKI) is a common complication in the critically ill. Current standard of care mainly relies on identification of patients at risk, haemodynamic optimization, avoidance of nephrotoxicity and the use of renal replacement therapy (RRT) in established AKI. The detection of early biomarkers of renal tissue damage is a recent development that allows amending the late and insensitive diagnosis with current AKI criteria. Increasing evidence suggests that the consequences of an episode of AKI extend long beyond the acute hospitalization. Citrate has been established as the anticoagulant of choice for continuous RRT. Conflicting results have been published on the optimal timing of RRT and on the renoprotective effect of remote ischaemic preconditioning. Recent research has contradicted that acute tubular necrosis is the common pathology in AKI, that septic AKI is due to global kidney hypoperfusion, that aggressive fluid therapy benefits the kidney, that vasopressor therapy harms the kidney and that high doses of RRT improve outcome. Remaining uncertainties include the impact of aetiology and clinical context on pathophysiology, therapy and prognosis, the clinical benefit of biomarker-driven interventions, the optimal mode of RRT to improve short- and long-term patient and kidney outcomes, the contribution of AKI to failure of other organs and the optimal approach for assessing and promoting renal recovery. Based on the established gaps in current knowledge the trials that must have priority in the coming 10 years are proposed together with the definition of appropriate clinical endpoints.
Keywords: Acute kidney injury; Biomarkers; Fluid therapy; Renal replacement therapy; Research agenda; Trial endpoints.
Conflict of interest statement
MS declares no conflicts of interest.
Figures
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–R212. - PMC - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury: AKI definition. Kidney Intern Suppl. 2012;2:19–36.
-
- Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, Mintz GS, Lansky AJ, Moses JW, Stone GW, Leon MB, Dangas G. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393–1399. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
