

Prostate cancer screening practices in a large, integrated health system: 2007-2014
- PMID: 28139034
- PMCID: PMC5515687
- DOI: 10.1111/bju.13793
Prostate cancer screening practices in a large, integrated health system: 2007-2014
Abstract
Objectives: To assess prostate cancer screening practices in primary care since the initial United States Preventive Services Task Force (USPSTF) recommendation against prostate-specific antigen (PSA) testing for older men, and to assess primary provider variation associated with prostate cancer screening.
Patients and methods: Our study population included 160 211 men aged ≥40 years with at least one visit to a primary care clinic in any of the study years in a large, integrated health system. We conducted a retrospective cohort study using electronic medical record data from January 2007 to December 2014. Yearly rates of screening PSA testing by primary care providers (PCPs), rates of re-screening, and rates of prostate biopsies were assessed.
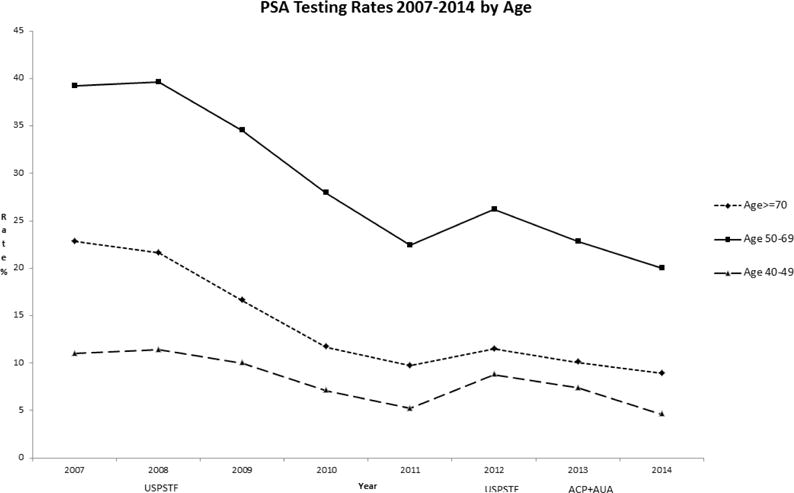
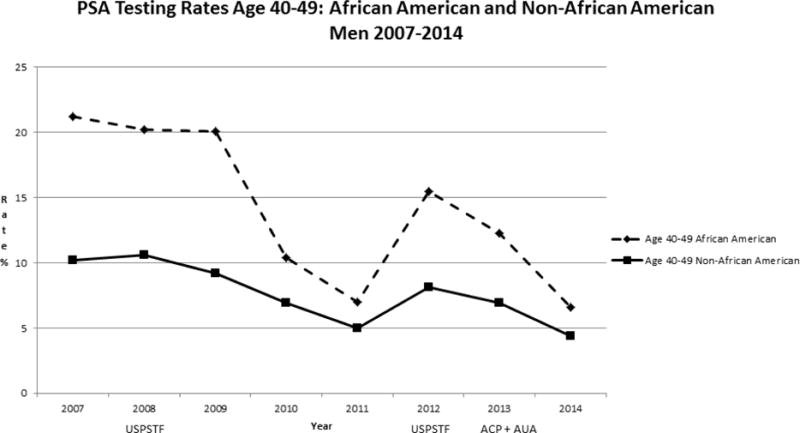
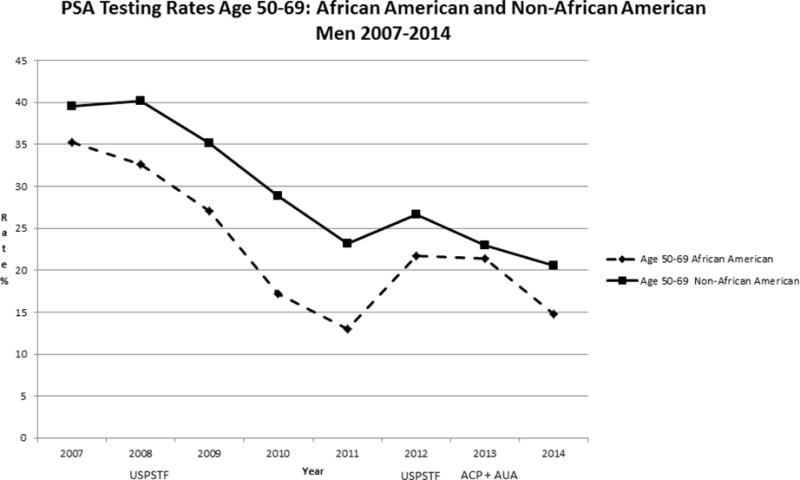
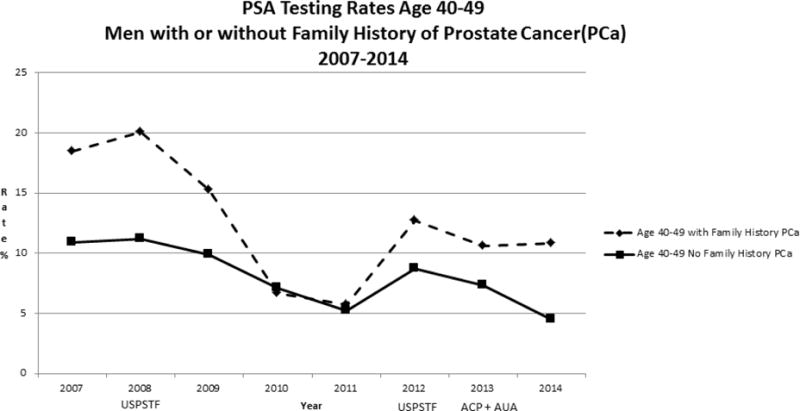
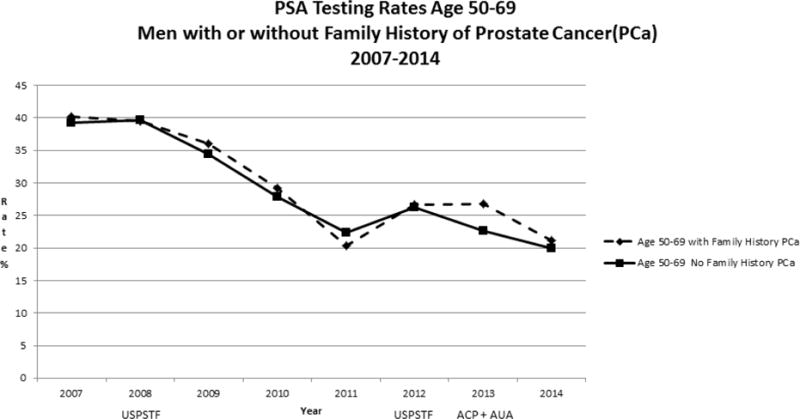
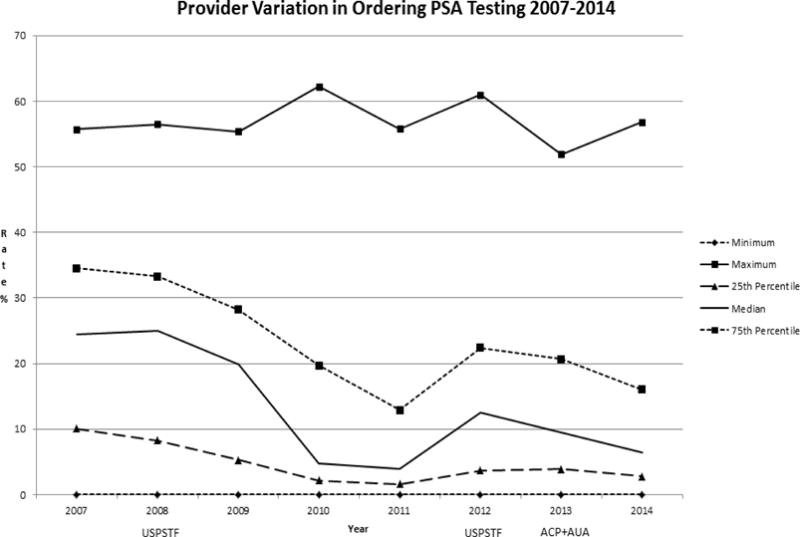
Results: Annual PSA-screening testing declined from 2007 to 2014 in all age groups, as did biennial and quadrennial screening. Yearly rates declined for men aged ≥70 years, from 22.8% to 8.9%; ages 50-69 years, from 39.2% to 20%; and ages 40-49 years, from 11% to 4.6%. Overall rates were lower for African-American (A-A) men vs non-A-A men; for men with a family history of prostate cancer, rates were similar or slightly higher than for those without a family history. PCP variation associated with ordering of PSA testing did not substantially change after the USPSTF recommendations. While the number of men screened and rates of follow-up prostate cancer screening declined in 2011-2014 compared to 2007-2010, similar re-screening rates were noted for men aged 45-75 years with initial PSA levels of <1 ng/mL or 1-3 ng/mL in both the earlier and later cohorts. For men aged >75 years with initial PSA levels of <3 ng/mL screened in both cohorts, follow-up screening rates were similar. Rates of prostate biopsy declined for men aged ≥70 years in 2014 compared to 2007. For men who had PSA screening, rates of first prostate biopsy increased in later years for A-A men and men with a family history of prostate cancer.
Conclusions: Prostate cancer screening declined from 2007 to 2014 even in higher-risk groups and follow-up screening rates were not related to previous PSA level. However, rates of first prostate biopsy in men who were screened with a PSA test were higher for men with an increased risk of prostate cancer in later years. Variation in PSA testing was noted among PCPs. Future work should further explore sources of variation in screening practices and implementation of risk-based strategies for prostate cancer screening in primary care.
Keywords: #PCSM; #ProstateCancer; cancer screening; primary care.
© 2017 The Authors BJU International © 2017 BJU International Published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Seniority of primary care physicians is associated with a decrease in PSA ordering habits in the years surrounding the United States Preventative Services Task Force recommendation against PSA screening.Urol Oncol. 2018 Nov;36(11):500.e21-500.e27. doi: 10.1016/j.urolonc.2018.07.011. Epub 2018 Sep 18. Urol Oncol. 2018. PMID: 30241954
-
Primary care physician PSA screening practices before and after the final U.S. Preventive Services Task Force recommendation.Urol Oncol. 2014 Jan;32(1):41.e23-30. doi: 10.1016/j.urolonc.2013.04.013. Epub 2013 Aug 2. Urol Oncol. 2014. PMID: 23911680
-
National Prostate Cancer Screening Rates After the 2012 US Preventive Services Task Force Recommendation Discouraging Prostate-Specific Antigen-Based Screening.J Clin Oncol. 2015 Aug 1;33(22):2416-23. doi: 10.1200/JCO.2015.61.6532. Epub 2015 Jun 8. J Clin Oncol. 2015. PMID: 26056181
-
Impact of the United States Preventive Services Task Force 'D' recommendation on prostate cancer screening and staging.Curr Opin Urol. 2017 May;27(3):205-209. doi: 10.1097/MOU.0000000000000383. Curr Opin Urol. 2017. PMID: 28221220 Review.
-
Relevance of total PSA and free PSA prescriptions.Ann Biol Clin (Paris). 2018 Dec 1;76(6):659-663. doi: 10.1684/abc.2018.1392. Ann Biol Clin (Paris). 2018. PMID: 30543191 Review. English.
Cited by
-
Prostate Cancer: Community Education and Disparities in Diagnosis and Treatment.Oncologist. 2021 Jul;26(7):537-548. doi: 10.1002/onco.13749. Epub 2021 Mar 22. Oncologist. 2021. PMID: 33683758 Free PMC article.
-
Association between platelet‑to‑lymphocyte ratio and serum prostate specific antigen.Mol Clin Oncol. 2023 Dec 12;20(2):10. doi: 10.3892/mco.2023.2708. eCollection 2024 Feb. Mol Clin Oncol. 2023. PMID: 38213661 Free PMC article.
-
Use of the prostate-specific antigen (PSA) test in the United States for men age ≥65, 1999-2015: Implications for practice interventions.Cancer Rep (Hoboken). 2021 Aug;4(4):e1352. doi: 10.1002/cnr2.1352. Epub 2021 May 1. Cancer Rep (Hoboken). 2021. PMID: 33932150 Free PMC article.
-
Changes in the outcome of prostate biopsies after preventive task force recommendation against prostate-specific antigen screening.BMC Urol. 2018 Aug 20;18(1):69. doi: 10.1186/s12894-018-0384-x. BMC Urol. 2018. PMID: 30126402 Free PMC article.
-
The use of electronic health records to inform cancer surveillance efforts: a scoping review and test of indicators for public health surveillance of cancer prevention and control.BMC Med Inform Decis Mak. 2022 Apr 6;22(1):91. doi: 10.1186/s12911-022-01831-8. BMC Med Inform Decis Mak. 2022. PMID: 35387655 Free PMC article.
References
-
- SEER Stat Fact Sheets: Prostate Cancer [Internet] Surveillance, Epidemiology, and End Results Program. Available from: http://seer.cancer.gov/statfacts/html/prost.html.
-
- Penson DF, McLerran D, Feng Z, Li L, Albertsen PC, Gilliland FD, et al. 5-year urinary and sexual outcomes after radical prostatectomy: results from the prostate cancer outcomes study. J Urol. 2005 May;173(5):1701–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
