

Ruxolitinib reverses dysregulated T helper cell responses and controls autoimmunity caused by a novel signal transducer and activator of transcription 1 (STAT1) gain-of-function mutation
- PMID: 28139313
- PMCID: PMC5482293
- DOI: 10.1016/j.jaci.2016.11.022
Ruxolitinib reverses dysregulated T helper cell responses and controls autoimmunity caused by a novel signal transducer and activator of transcription 1 (STAT1) gain-of-function mutation
Abstract
Background: Gain-of-function (GOF) mutations in the human signal transducer and activator of transcription 1 (STAT1) manifest in immunodeficiency and autoimmunity with impaired TH17 cell differentiation and exaggerated responsiveness to type I and II interferons. Allogeneic bone marrow transplantation has been attempted in severely affected patients, but outcomes have been poor.
Objective: We sought to define the effect of increased STAT1 activity on T helper cell polarization and to investigate the therapeutic potential of ruxolitinib in treating autoimmunity secondary to STAT1 GOF mutations.
Methods: We used in vitro polarization assays, as well as phenotypic and functional analysis of STAT1-mutated patient cells.
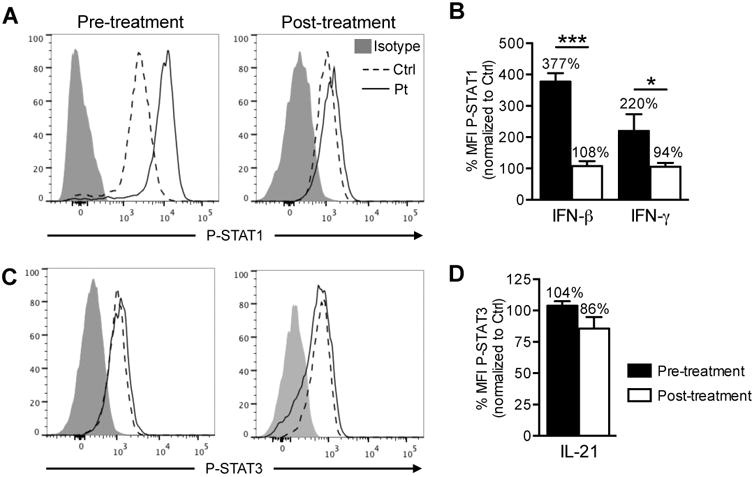
Results: We report a child with a novel mutation in the linker domain of STAT1 who had life-threatening autoimmune cytopenias and chronic mucocutaneous candidiasis. Naive lymphocytes from the affected patient displayed increased TH1 and follicular T helper cell and suppressed TH17 cell responses. The mutation augmented cytokine-induced STAT1 phosphorylation without affecting dephosphorylation kinetics. Treatment with the Janus kinase 1/2 inhibitor ruxolitinib reduced hyperresponsiveness to type I and II interferons, normalized TH1 and follicular T helper cell responses, improved TH17 differentiation, cured mucocutaneous candidiasis, and maintained remission of immune-mediated cytopenias.
Conclusions: Autoimmunity and infection caused by STAT1 GOF mutations are the result of dysregulated T helper cell responses. Janus kinase inhibitor therapy could represent an effective targeted treatment for long-term disease control in severely affected patients for whom hematopoietic stem cell transplantation is not available.
Keywords: IFN-γ; STAT1 gain of function; T helper cell polarization; T(H)1 cell; T(H)17 cell; autoimmunity; follicular T helper cell; ruxolitinib.
Copyright © 2016 American Academy of Allergy, Asthma & Immunology. All rights reserved.
Figures






References
-
- Subramaniam PS, Torres BA, Johnson HM. So many ligands, so few transcription factors: a new paradigm for signaling through the STAT transcription factors. Cytokine. 2001;15:175–87. - PubMed
-
- vdV FL. STAT1 Mutations in Autosomal Dominant Chronic Mucocutaneous Candidiasis. N Engl J Med. 2011:54–61. - PubMed
-
- Hori T, Ohnishi H, Teramoto T, Tsubouchi K, Naiki T, Hirose Y, et al. Autosomal-dominant chronic mucocutaneous candidiasis with STAT1-mutation can be complicated with chronic active hepatitis and hypothyroidism. J Clin Immunol. 2012;32:1213–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
