

Review
doi: 10.1038/ajg.2016.610.
Epub 2017 Jan 31.
A Multidisciplinary Approach to Pancreas Cancer in 2016: A Review
Affiliations
- PMID: 28139655
- PMCID: PMC5659272
- DOI: 10.1038/ajg.2016.610
Item in Clipboard
Review
A Multidisciplinary Approach to Pancreas Cancer in 2016: A Review
Am J Gastroenterol.
2017 Apr.
Abstract
In this article, we review our multidisciplinary approach for patients with pancreatic cancer. Specifically, we review the epidemiology, diagnosis and staging, biliary drainage techniques, selection of patients for surgery, chemotherapy, radiation therapy, and discuss other palliative interventions. The areas of active research investigation and where our knowledge is limited are emphasized.
Conflict of interest statement
Figures
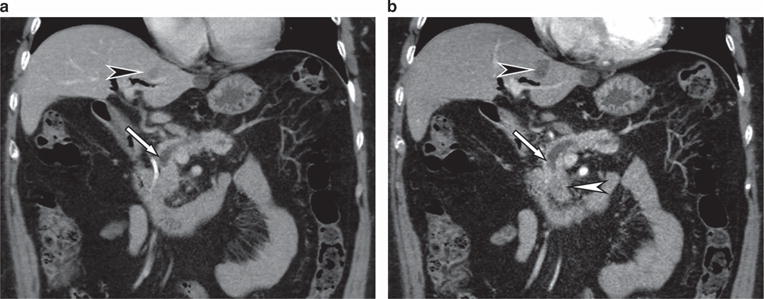
A 67-year-old female presents with persistent abdominal pain and weight loss. (a) Axial computed tomography (CT) performed with thick slices (5 mm) at an outside institution shows an abrupt cutoff of the main pancreatic duct (arrow). No obvious pancreatic head mass was seen. In addition, an ill-defined liver lesion was seen (black arrowhead). (b) Axial CT at our institution performed as per the pancreas protocol with thin slices (3 mm) in parenchymal phase shows the duct cutoff (arrow) caused by an ill-defined low-density pancreatic head mass (white arrowhead). The liver lesion (black arrowhead) is shown to have a clear outline and was diagnosed as a benign cyst. The patient underwent pancreaticoduodenectomy for resectable ductal adenocarcinoma.
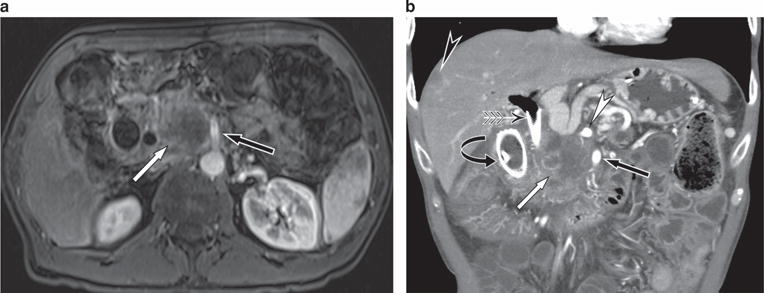
A 53-year-old male presents with painless jaundice. (a) Axial postgadolinium magnetic resonance imaging (MRI) shows a large mass in the pancreatic head (white arrow) closely applied to the superior mesenteric artery (SMA) (black arrow). The tumor was deemed unresectable because of the long length of contact with the SMA. (b) Coronal computed tomography (CT) performed 2 months later shows metal biliary (winged arrow) and duodenal (curved arrow) stents in place. There remains a large tumor (white arrow) that is closely applied to the SMA (black arrow) and celiac artery (white arrowhead). In addition, a liver metastases (black arrowhead) is seen.
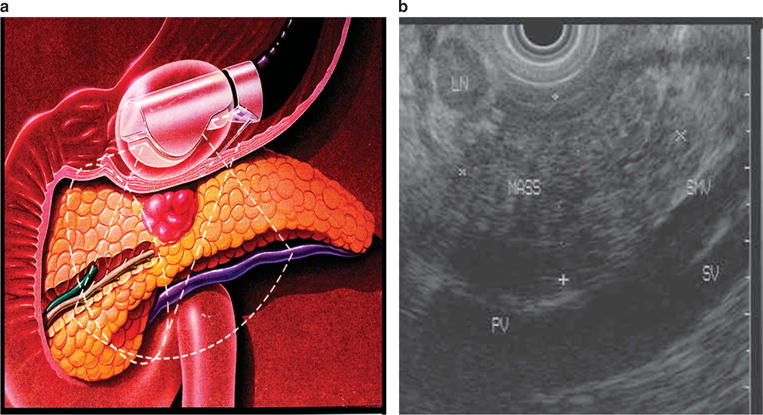
(a) Schematic illustration of a mass in the body of the pancreas. Endoscopic ultrasound evaluation of a patient with epigastric pain and weight loss, with computed tomography (CT) demonstrating a pancreas mass. (b) The pancreas mass is abutting the portal confluence.
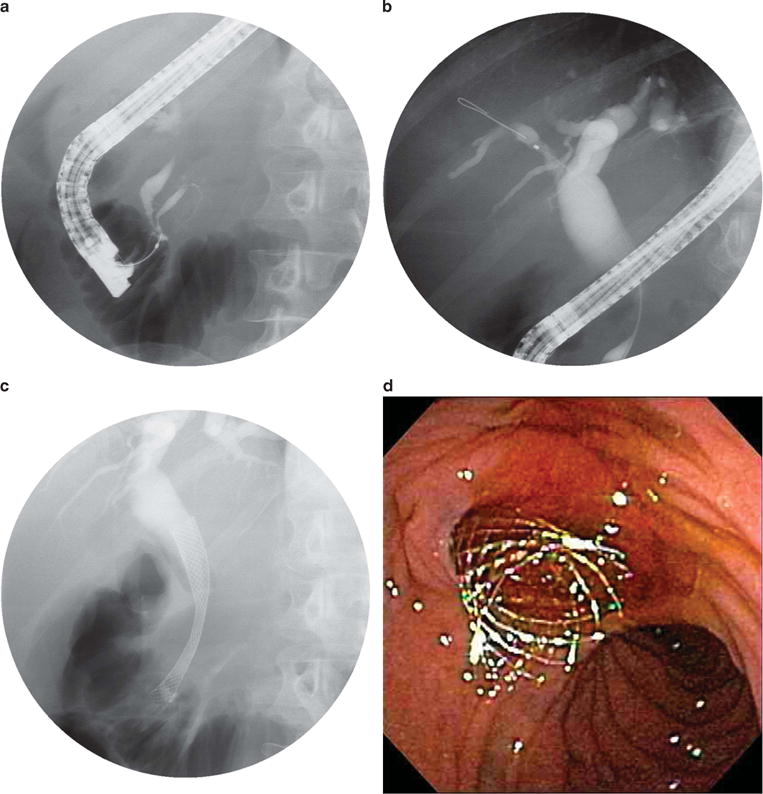
Endoscopic retrograde cholangiopancreatography (ERCP) images obtained in a 70-year-old man with abdominal pain, diarrhea, jaundice, and weight loss. Computed tomography (CT) scan reveals a head of pancreas mass. (a) Contrast injection reveals an obstructed pancreatic duct and distal bile duct stricture (“double-duct sign”). (b) Biliary dilation proximal to the biliary stricture. (c) Fluoroscopic image of a metal stent placed through the biliary stricture. (d) Endoscopic image of a metal stent placed through the biliary stricture, with subsequent bile flow.
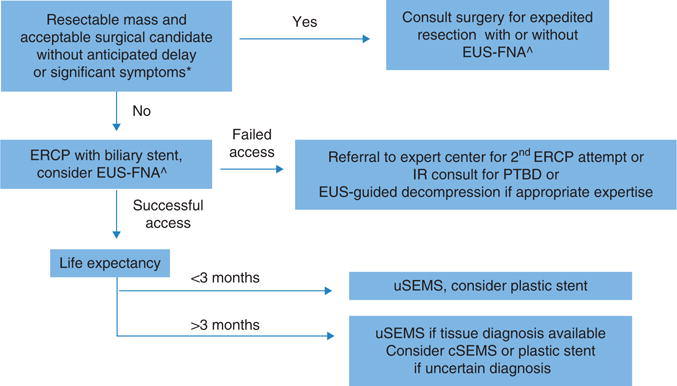
Algorithm for management of malignant biliary obstruction. *Patients with anticipated delays of surgery >2 weeks for work-up/stabilization of comorbidities should undergo preoperative decompression; significant symptoms=deep jaundice, refractory pruritus. ^Endoscopic ultrasound fine-needle aspiration (EUS-FNA) should be performed in patients with elevated suspicion for autoimmune pancreatitis or otherwise benign disease-causing obstruction, or for tissue confirmation before planned chemoradiotherapy. cSEMS, covered self-expandable metallic stent; PTBD, percutaneous transhepatic biliary decompression; uSEMS, uncovered self-expandable metallic stent.
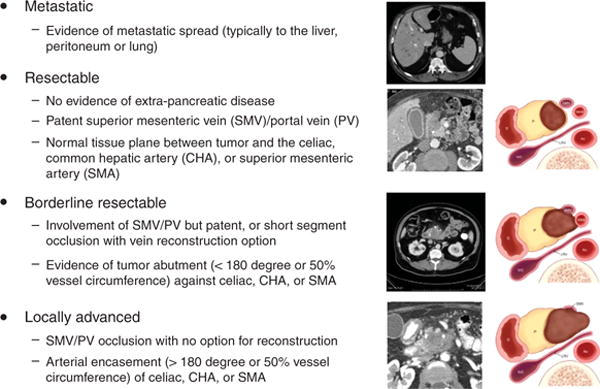
Computed tomography (CT) criteria for determining resectability of pancreatic ductal adenocarcinoma.
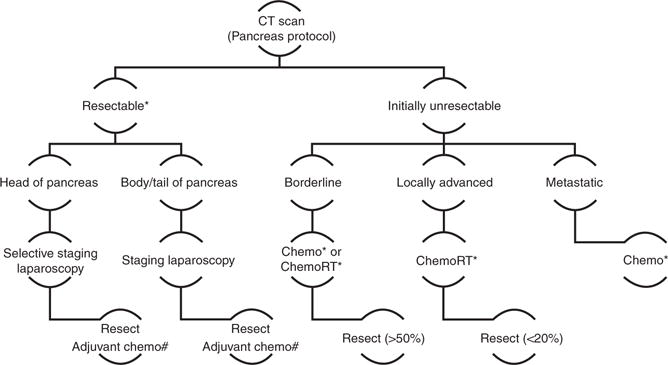
Approach to patients with pancreatic ductal adenocarcinoma after complete staging by computed tomography (CT). # Substitute ChemoRT for Chemo if R1 resection on final pathology. * Clinical trial offered for patients.
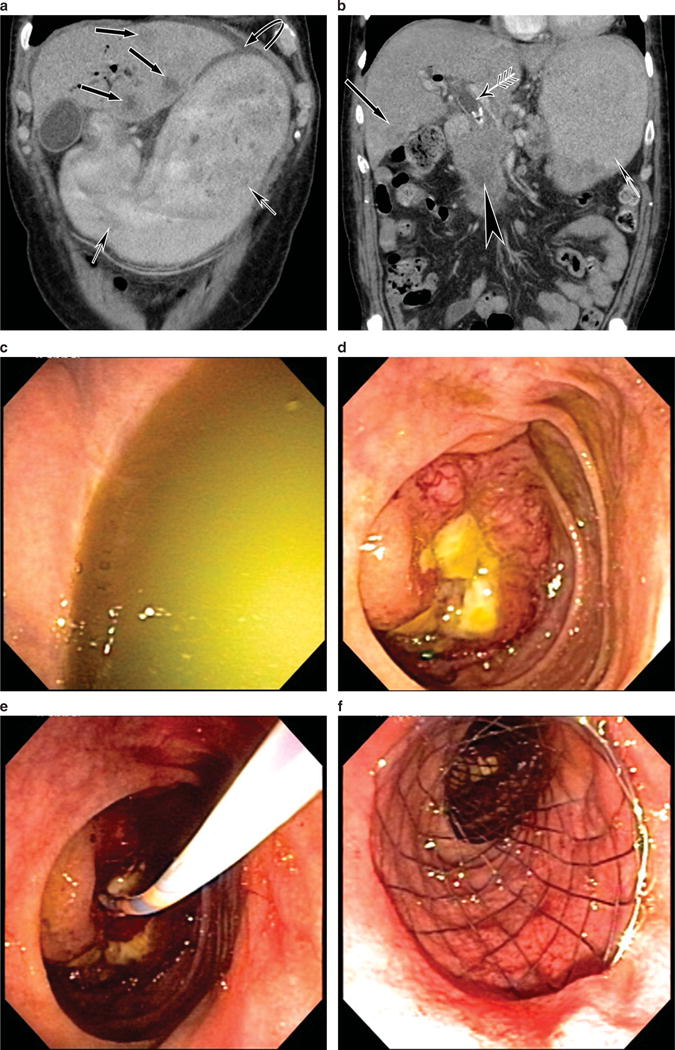
This patient with metastatic pancreas cancer presents with nausea and vomiting. (a) Computed tomography (CT) scan reveals liver metastases and a distended stomach. (b) CT scan reveals the pancreas mass, a dilated bile duct with stent in place, liver metastasis, and a distended fluid-filled stomach. (c) Endoscopic image of the fluid-filled stomach. (d) Duodenal obstruction by tumor. (e) Catheter and guidewire passage beyond the obstruction. (f) Duodenal stent placed.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975–2013. National Cancer Institute; Bethesda, MD: available at http://seer.cancer.gov/csr/1975_2013/, based on November 2015. SEER data submission, posted to the SEER website, April 2016.
-
- Raimondi S, Lowenfels AB, Morselli-Labate AM, et al. Pancreatic cancer in chronic pancreatitis: aetiology, incidence, and early detection. Best Pract Res Clin Gastro. 2010;24:349–58. - PubMed
-
- Lowenfels AB, Maisonneuve P, Cavallini G, et al. Pancreatitis and the risk of pancreatic cancer. N Engl J Med. 1993;328:1433–7. - PubMed
-
- Ben Q, Xu M, Ning X, et al. Diabetes mellitus and risk of pancreatic cancer: a meta-analysis of cohort studies. Eur J Cancer. 2011;47:1928–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
