

Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come
- PMID: 28140318
- PMCID: PMC5105038
- DOI: 10.3945/an.116.012765
Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come
Abstract
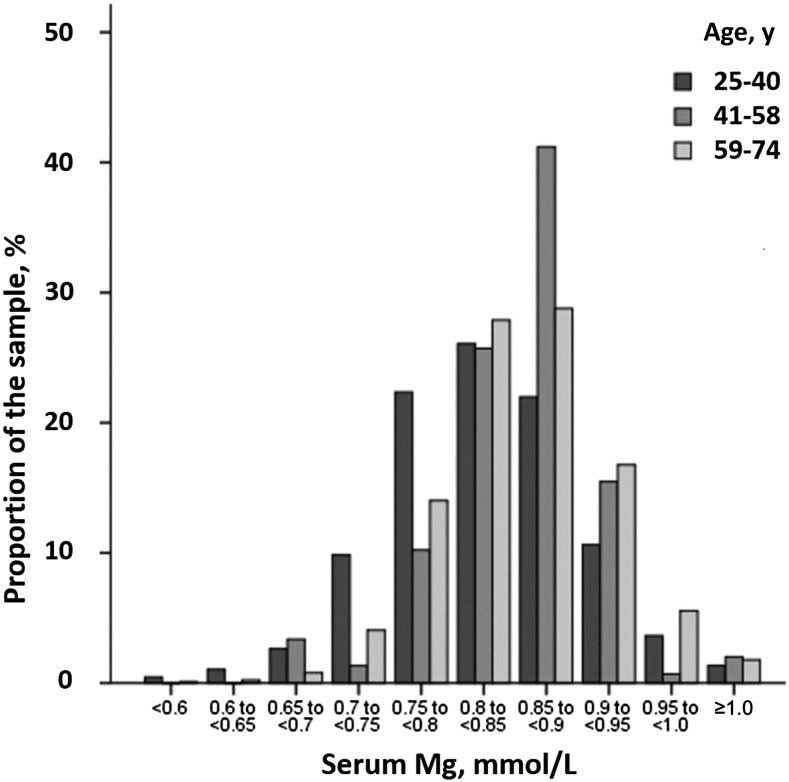
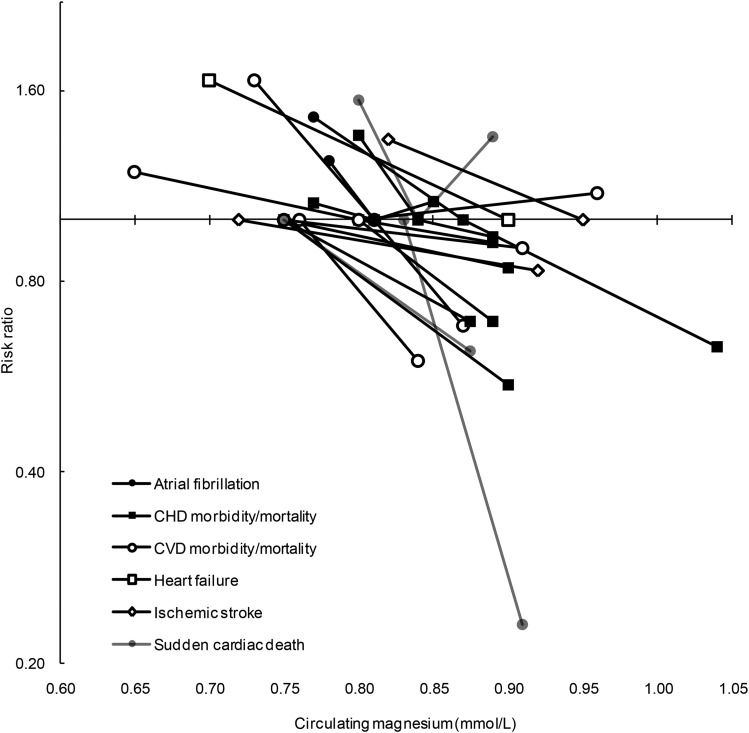
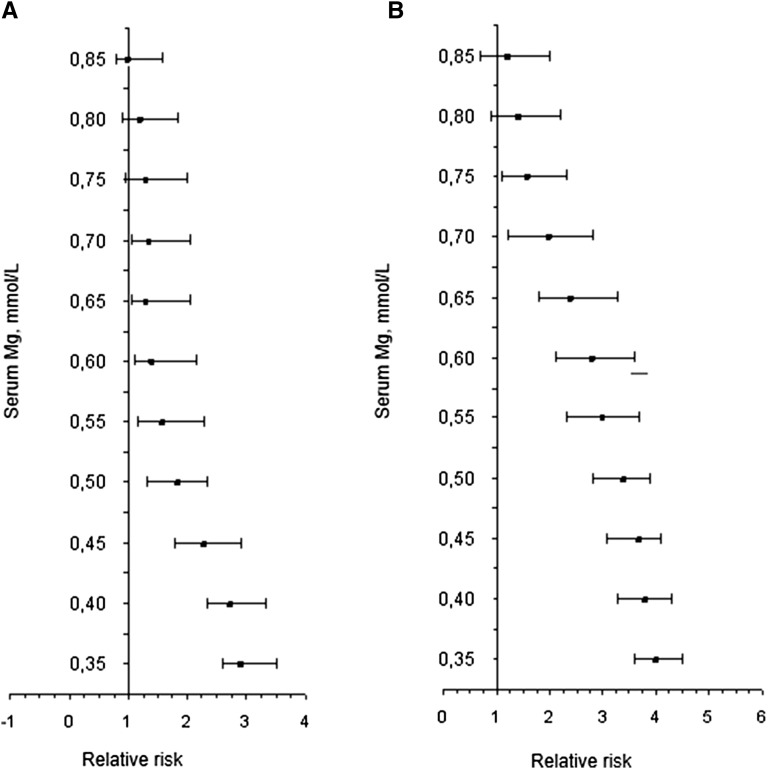
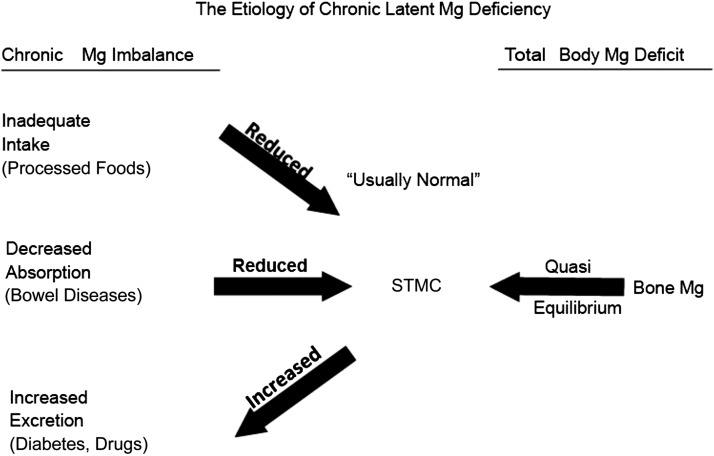
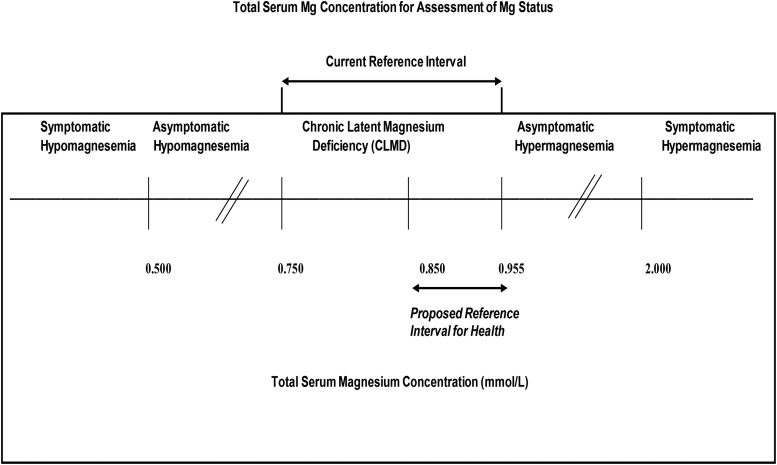
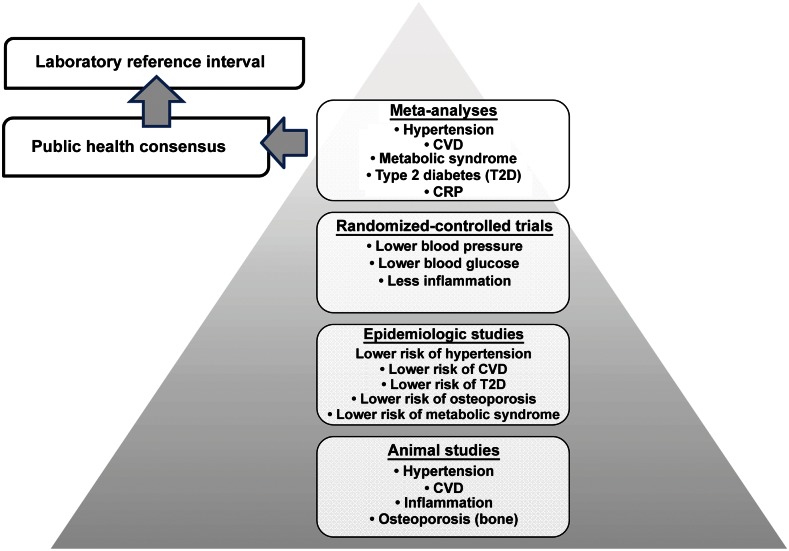
The 2015 Dietary Guidelines Advisory Committee indicated that magnesium was a shortfall nutrient that was underconsumed relative to the Estimated Average Requirement (EAR) for many Americans. Approximately 50% of Americans consume less than the EAR for magnesium, and some age groups consume substantially less. A growing body of literature from animal, epidemiologic, and clinical studies has demonstrated a varied pathologic role for magnesium deficiency that includes electrolyte, neurologic, musculoskeletal, and inflammatory disorders; osteoporosis; hypertension; cardiovascular diseases; metabolic syndrome; and diabetes. Studies have also demonstrated that magnesium deficiency is associated with several chronic diseases and that a reduced risk of these diseases is observed with higher magnesium intake or supplementation. Subclinical magnesium deficiency can exist despite the presentation of a normal status as defined within the current serum magnesium reference interval of 0.75-0.95 mmol/L. This reference interval was derived from data from NHANES I (1974), which was based on the distribution of serum magnesium in a normal population rather than clinical outcomes. What is needed is an evidenced-based serum magnesium reference interval that reflects optimal health and the current food environment and population. We present herein data from an array of scientific studies to support the perspective that subclinical deficiencies in magnesium exist, that they contribute to several chronic diseases, and that adopting a revised serum magnesium reference interval would improve clinical care and public health.
Keywords: chronic disease; magnesium deficiency; plasma magnesium; reference interval; serum magnesium.
© 2016 American Society for Nutrition.
Conflict of interest statement
4 Author disclosures: RB Costello, RJ Elin, A Rosanoff, TC Wallace, F Guerrero-Romero, A Hruby, PL Lutsey, FH Nielsen, M Rodriguez-Moran, Y Song, and LV Van Horn, no conflicts of interest.
Figures
References
-
- Moshfegh A, Goldman JD, Ahuja J, Rhodes D, LaComb R. What we eat in America, NHANES 2005–2006: usual nutrient intakes from food and water compared to 1997 Dietary Reference Intakes for vitamin D, calcium, phosphorus, and magnesium. Washington (DC): USDA; 2009.
-
- US Department of Health and Human Services. Scientific report of the 2015 Dietary Guidelines Advisory Committee [Internet]. [cited 2015 Oct 1]. Available from: http://health.gov/dietaryguidelines/2015-scientific-report.
-
- European Food Safety Authority. Scientific opinion on dietary reference values for magnesium. EFSA J 2015;13:4186.
-
- Jee SH, Miller ER III, Guallar E, Singh VK, Appel LJ, Klag MJ. The effect of magnesium supplementation on blood pressure: a meta-analysis of randomized clinical trials. Am J Hypertens 2002;15:691–6. - PubMed
-
- Dickinson HO, Nicolson DJ, Campbell F, Cook JV, Beyer FR, Ford GA, Mason J. Magnesium supplementation for the management of essential hypertension in adults. Cochrane Database Syst Rev 2006;3:CD004640. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
