

Head injury serum markers for assessing response to trauma: Design of the HeadSMART study
- PMID: 28140672
- PMCID: PMC6438171
- DOI: 10.1080/02699052.2016.1231344
Head injury serum markers for assessing response to trauma: Design of the HeadSMART study
Abstract
Background: Accurate diagnosis and risk stratification of traumatic brain injury (TBI) at time of presentation remains a clinical challenge. The Head Injury Serum Markers for Assessing Response to Trauma study (HeadSMART) aims to examine blood-based biomarkers for diagnosing and determining prognosis in TBI.
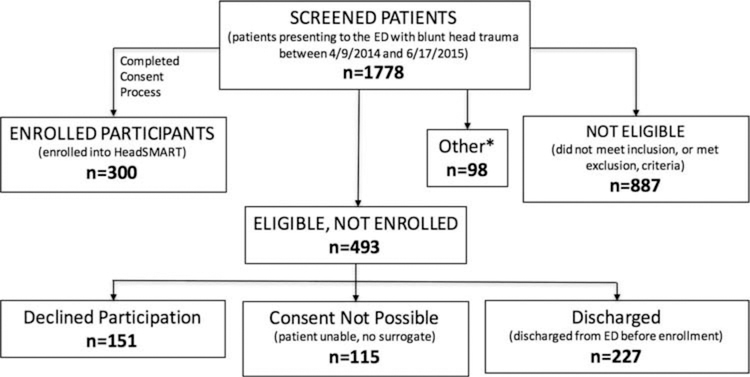
Methods: HeadSMART is a 6-month prospective cohort study comparing emergency department patients evaluated for TBI (exposure group) to (1) emergency department patients evaluated for traumatic injury without head trauma and (2) healthy persons. Study methods and characteristics of the first 300 exposure participants are discussed.
Results: Of the first 300 participants in the exposure arm, 70% met the American Congress of Rehabilitation Medicine criteria for TBI, with the majority (80.1%) classified as mild TBI. The majority of subjects in the exposure arm had Glasgow Coma Scale scores of 13-15 (98.0%), normal head computed tomography (81.3%) and no prior history of concussion (71.7%).
Conclusion: With systematic phenotyping, HeadSMART will facilitate diagnosis and risk-stratification of the heterogeneous group of individuals currently diagnosed with TBI.
Keywords: TBI; Traumatic brain injury; biomarkers; blunt head trauma.
Figures
Similar articles
-
Neuronal Biomarker Ubiquitin C-Terminal Hydrolase Detects Traumatic Intracranial Lesions on Computed Tomography in Children and Youth with Mild Traumatic Brain Injury.J Neurotrauma. 2017 Jul 1;34(13):2132-2140. doi: 10.1089/neu.2016.4806. Epub 2017 Apr 18. J Neurotrauma. 2017. PMID: 28158951 Free PMC article.
-
Simultaneous head and facial computed tomography scans for assessing facial fractures in patients with traumatic brain injury.Injury. 2017 Jul;48(7):1417-1422. doi: 10.1016/j.injury.2017.04.046. Epub 2017 Apr 24. Injury. 2017. PMID: 28455003
-
Point-of-Care Platform Blood Biomarker Testing of Glial Fibrillary Acidic Protein versus S100 Calcium-Binding Protein B for Prediction of Traumatic Brain Injuries: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study.J Neurotrauma. 2020 Dec 1;37(23):2460-2467. doi: 10.1089/neu.2020.7140. Epub 2020 Sep 14. J Neurotrauma. 2020. PMID: 32854584 Free PMC article.
-
[Diagnostic approach to the mild head trauma of the adult in Emergency Medicine: between biomarkers and imaging].Recenti Prog Med. 2013 Mar;104(3):120-32. doi: 10.1701/1255.13861. Recenti Prog Med. 2013. PMID: 23548957 Review. Italian.
-
Traumatic brain injury detection performance of the infant scalp score in children younger than 2 years in the pediatric emergency department.Eur J Trauma Emerg Surg. 2023 Aug;49(4):1673-1681. doi: 10.1007/s00068-022-02085-9. Epub 2022 Sep 3. Eur J Trauma Emerg Surg. 2023. PMID: 36056932 Review.
Cited by
-
Poor sleep is linked to impeded recovery from traumatic brain injury.Sleep. 2018 Oct 1;41(10):zsy147. doi: 10.1093/sleep/zsy147. Sleep. 2018. PMID: 30053263 Free PMC article.
-
Derivation of a Three Biomarker Panel to Improve Diagnosis in Patients with Mild Traumatic Brain Injury.Front Neurol. 2017 Nov 30;8:641. doi: 10.3389/fneur.2017.00641. eCollection 2017. Front Neurol. 2017. PMID: 29250027 Free PMC article.
-
Prevalence of Incomplete Functional and Symptomatic Recovery among Patients with Head Injury but Brain Injury Debatable.J Neurotrauma. 2017 Apr 15;34(8):1531-1538. doi: 10.1089/neu.2016.4723. Epub 2016 Dec 20. J Neurotrauma. 2017. PMID: 27784200 Free PMC article.
-
Influence of study population definition on the effect of age on outcomes after blunt head trauma.Brain Inj. 2018;32(13-14):1725-1730. doi: 10.1080/02699052.2018.1520301. Epub 2018 Sep 19. Brain Inj. 2018. PMID: 30230916 Free PMC article.
-
A Precision Medicine Agenda in Traumatic Brain Injury.Front Pharmacol. 2022 Mar 16;13:713100. doi: 10.3389/fphar.2022.713100. eCollection 2022. Front Pharmacol. 2022. PMID: 35370671 Free PMC article. Review.
References
-
- Centers for Disease Control and Prevention (CDC) National Center for Health Statistics. 2010. \,; 2010 National Hospital Ambulatory Medical Care Survey (NHAMCS), 2010.
-
- Centers for Disease Control and Prevention(CDC) NCfIPaC. 2003. Report to Congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Atlanta, GA: Centers for Disease Control and Prevention.
-
- Kim E, Lauterbach EC, Reeve A, Arciniegas DB, Coburn KL, Mendez MF, Rummans TA, Coffey EC, Research ACo. 2007. Neuropsychiatric complications of traumatic brain injury: a critical review of the literature (a report by the ANPA Committee on Research). J Neuropsychiatry Clin Neurosci 19(2):106–27. - PubMed
-
- Rao V, Koliatsos V, Ahmed F, Lyketsos C, Kortte K. 2015. Neuropsychiatric disturbances associated with traumatic brain injury: a practical approach to evaluation and management. Semin Neurol 35(1):64–82. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous