

New film-coated tablet formulation of deferasirox is well tolerated in patients with thalassemia or lower-risk MDS: Results of the randomized, phase II ECLIPSE study
- PMID: 28142202
- PMCID: PMC6585741
- DOI: 10.1002/ajh.24668
New film-coated tablet formulation of deferasirox is well tolerated in patients with thalassemia or lower-risk MDS: Results of the randomized, phase II ECLIPSE study
Abstract
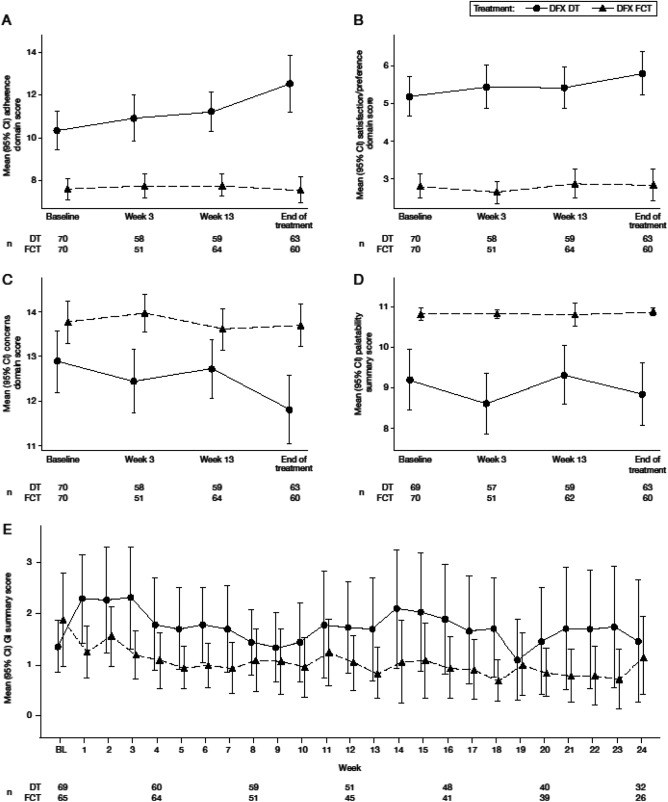
Once-daily deferasirox dispersible tablets (DT) have a well-defined safety and efficacy profile and, compared with parenteral deferoxamine, provide greater patient adherence, satisfaction, and quality of life. However, barriers still exist to optimal adherence, including gastrointestinal tolerability and palatability, leading to development of a new film-coated tablet (FCT) formulation that can be swallowed with a light meal, without the need to disperse into a suspension prior to consumption. The randomized, open-label, phase II ECLIPSE study evaluated the safety of deferasirox DT and FCT formulations over 24 weeks in chelation-naïve or pre-treated patients aged ≥10 years, with transfusion-dependent thalassemia or IPSS-R very-low-, low-, or intermediate-risk myelodysplastic syndromes. One hundred seventy-three patients were randomized 1:1 to DT (n = 86) or FCT (n = 87). Adverse events (overall), consistent with the known deferasirox safety profile, were reported in similar proportions of patients for each formulation (DT 89.5%; FCT 89.7%), with a lower frequency of severe events observed in patients receiving FCT (19.5% vs. 25.6% DT). Laboratory parameters (serum creatinine, creatinine clearance, alanine aminotransferase, aspartate aminotransferase and urine protein/creatinine ratio) generally remained stable throughout the study. Patient-reported outcomes showed greater adherence and satisfaction, better palatability and fewer concerns with FCT than DT. Treatment compliance by pill count was higher with FCT (92.9%) than with DT (85.3%). This analysis suggests deferasirox FCT offers an improved formulation with enhanced patient satisfaction, which may improve adherence, thereby reducing frequency and severity of iron overload-related complications.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
ATT reports receiving research funding and honoraria from Novartis; RO reports receiving honoraria from Novartis and Apopharma; SP reports receiving honoraria from Novartis; AKa reports receiving research funding and participating in advisory boards and educational forums sponsored by Novartis; AKo reports receiving honoraria from Novartis, Amgen, and Janssen, and consultancy for Gilead, Roche, and Celgene; JBP reports consultancy, receiving research grant funding and honoraria from Novartis Pharmaceuticals, consultancy and honoraria from Shire, and consultancy for Celgene. JBP is supported by the NIHR University College London Hospitals Biomedical Research Centre; AC, MW, RMH, and VH were full‐time employees of Novartis at the time of these analyses; A‐SG and GBR have no relevant conflicts of interest to disclose.
Figures
References
-
- Gabutti V, Piga A. Results of long‐term iron‐chelating therapy. Acta Haematol. 1996;95:26–36. - PubMed
-
- Delea TE, Edelsberg J, Sofrygin O, et al. Consequences and costs of noncompliance with iron chelation therapy in patients with transfusion‐dependent thalassemia: a literature review. Transfusion. 2007;47:1919–1929. - PubMed
-
- Escudero‐Vilaplana V, Garcia‐Gonzalez X, Osorio‐Prendes S, et al. Impact of medication adherence on the effectiveness of deferasirox for the treatment of transfusional iron overload in myelodysplastic syndrome. J Clin Pharm Ther. 2016;41:59–63. - PubMed
-
- Brittenham GM, Griffith PM, Nienhuis AW, et al. Efficacy of deferoxamine in preventing complications of iron overload in patients with thalassemia major. N Engl J Med. 1994;331:567–573. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous