

Retrospective case-control non-inferiority analysis of intravenous lidocaine in a colorectal surgery enhanced recovery program
- PMID: 28143397
- PMCID: PMC5282801
- DOI: 10.1186/s12871-017-0306-6
Retrospective case-control non-inferiority analysis of intravenous lidocaine in a colorectal surgery enhanced recovery program
Abstract
Background: Enhanced recovery after surgery (ERAS) programs typically utilizes multi-modal analgesia to reduce perioperative opioid consumption. Systemic lidocaine is used in several of these ERAS algorithms and has been shown to reduce opioid use after colorectal surgery. However it is unclear how much the other components of an ERAS protocol contribute to the final outcome. Using a noninferiority analysis we sought to assess the role of perioperative lidocaine in an ERAS program for colorectal surgery, using pain and opioid consumption as outcomes.
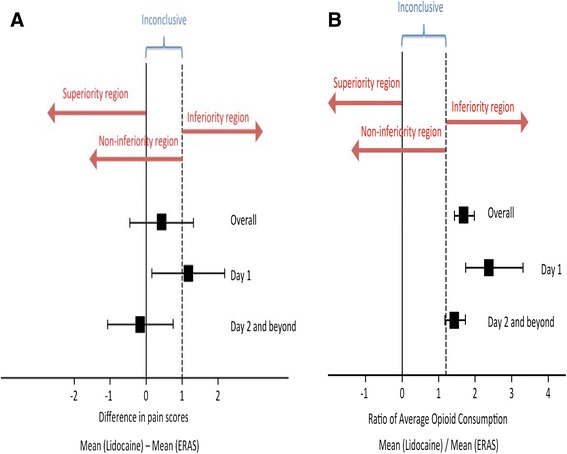
Methods: We conducted a retrospective review of patients who had received intravenous lidocaine perioperatively during colorectal surgery. We matched them with patients who were managed using a multi-component ERAS protocol, which included perioperative lidocaine. We tested a joint hypothesis of noninferiority of lidocaine infusion to ERAS protocol in postoperative pain scores and opioid consumption. We assigned a noninferiority margin of 1 point (on an 11-point numerical rating scale) difference in pain and a ratio [mean (lidocaine) / mean (ERAS)] of 1.2 in opioid consumption, respectively.
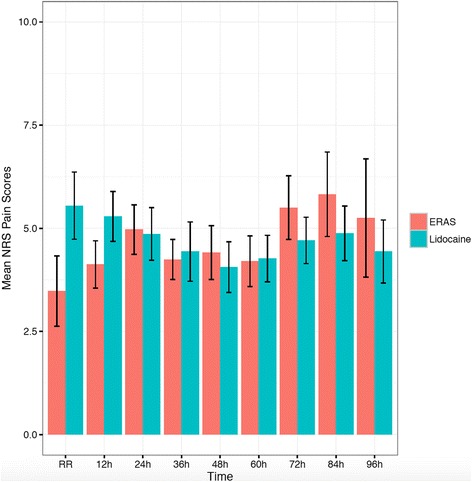
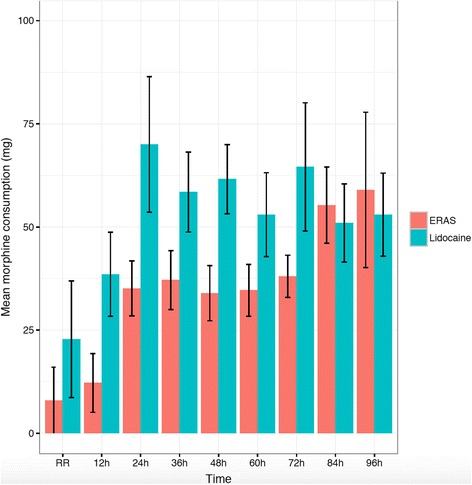
Results: Fifty-two patients in the lidocaine group were matched with patients in the ERAS group. With regards to opioid consumption, in the overall [1.68 (1.43-1.98)] [odds ratio (95% confidence interval)] analysis and on postoperative day (POD) 1 [2.38 (1.74-3.31)] lidocaine alone was inferior to multi-modal analgesia. On POD 2 and beyond, although the mean odds ratio for opioid consumption was 1.43 [1.43 (1.17-1.73)], the lower limit extended beyond the pre-defined cut-off of 1.2, rendering the outcome inconclusive. For pain scores lidocaine is non-inferior to ERAS [-0.17 (-1.08-0.74)] on POD 2 and beyond. Pain scores on POD 1 and in the overall cohort were inconclusive based on the noninferiority analysis.
Conclusions: The addition of a multi-component ERAS protocol to intravenous lidocaine incrementally reduces opioid consumption, most evident on POD 1. For pain scores the data is inconclusive on POD 1, however on POD 2 and beyond lidocaine alone is non-inferior to an ERAS program with lidocaine. Opioid-related complications, including return of bowel function, were not different between the groups despite reduced opioid use in the ERAS group.
Keywords: Colorectal Surgery; Enhanced Recovery After Surgery; Lidocaine; Opioid Consumption; Pain Scores.
Figures
Similar articles
-
A Clinical Comparison of Intravenous and Epidural Local Anesthetic for Major Abdominal Surgery.Reg Anesth Pain Med. 2016 Jan-Feb;41(1):28-36. doi: 10.1097/AAP.0000000000000332. Reg Anesth Pain Med. 2016. PMID: 26650426 Free PMC article.
-
Transversus abdominis plane block versus perioperative intravenous lidocaine versus patient-controlled intravenous morphine for postoperative pain control after laparoscopic colorectal surgery: study protocol for a prospective, randomized, double-blind controlled clinical trial.Trials. 2014 Dec 4;15:476. doi: 10.1186/1745-6215-15-476. Trials. 2014. PMID: 25472808 Free PMC article. Clinical Trial.
-
Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery.Anesth Analg. 2012 Aug;115(2):262-7. doi: 10.1213/ANE.0b013e318257a380. Epub 2012 May 14. Anesth Analg. 2012. PMID: 22584558 Clinical Trial.
-
Meta-analysis of the effect of perioperative intravenous lidocaine on return of gastrointestinal function after colorectal surgery.Tech Coloproctol. 2019 Jan;23(1):15-24. doi: 10.1007/s10151-019-1927-1. Epub 2019 Feb 5. Tech Coloproctol. 2019. PMID: 30721376 Free PMC article.
-
Intravenous lidocaine.Best Pract Res Clin Anaesthesiol. 2017 Dec;31(4):513-521. doi: 10.1016/j.bpa.2017.05.005. Epub 2017 May 30. Best Pract Res Clin Anaesthesiol. 2017. PMID: 29739540 Review.
Cited by
-
Thoracoscopic Intercostal Nerve Block with Cocktail Analgesics for Pain Control After Video-Assisted Thoracoscopic Surgery: A Prospective Cohort Study.J Pain Res. 2024 Mar 18;17:1183-1196. doi: 10.2147/JPR.S446951. eCollection 2024. J Pain Res. 2024. PMID: 38524689 Free PMC article.
-
Effect of Multimodal Analgesia on Opioid Use After Open Ventral Hernia Repair.J Gastrointest Surg. 2017 Oct;21(10):1692-1699. doi: 10.1007/s11605-017-3529-4. Epub 2017 Aug 14. J Gastrointest Surg. 2017. PMID: 28808868
-
Designing the ideal perioperative pain management plan starts with multimodal analgesia.Korean J Anesthesiol. 2018 Oct;71(5):345-352. doi: 10.4097/kja.d.18.00217. Epub 2018 Aug 24. Korean J Anesthesiol. 2018. PMID: 30139215 Free PMC article.
-
Intravenous Infusion of Lidocaine for Bowel Function Recovery After Major Colorectal Surgery: A Critical Appraisal Through Updated Meta-Analysis, Trial Sequential Analysis, Certainty of Evidence, and Meta-Regression.Front Med (Lausanne). 2022 Jan 27;8:759215. doi: 10.3389/fmed.2021.759215. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35155463 Free PMC article.
-
Role of Multimodal Analgesia in the Evolving Enhanced Recovery after Surgery Pathways.Medicina (Kaunas). 2018 Apr 23;54(2):20. doi: 10.3390/medicina54020020. Medicina (Kaunas). 2018. PMID: 30344251 Free PMC article. Review.
References
-
- Thiele RH, Rea KM, Turrentine FE, Friel CM, Hassinger TE, McMurry TL, Goudreau BJ, Umapathi BA, Kron IL, Sawyer RG, et al. Standardization of care: impact of an enhanced recovery protocol on length of stay, complications, and direct costs after colorectal surgery. Journal of the American College of Surgeons. 2015;220(4):430–443. doi: 10.1016/j.jamcollsurg.2014.12.042. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
