

Gait disorders in the elderly and dual task gait analysis: a new approach for identifying motor phenotypes
- PMID: 28143497
- PMCID: PMC5282774
- DOI: 10.1186/s12984-017-0218-1
Gait disorders in the elderly and dual task gait analysis: a new approach for identifying motor phenotypes
Abstract
Background: Gait disorders and gait analysis under single and dual-task conditions are topics of great interest, but very few studies have looked for the relevance of gait analysis under dual-task conditions in elderly people on the basis of a clinical approach.
Methods: An observational study including 103 patients (mean age 76.3 ± 7.2, women 56%) suffering from gait disorders or memory impairment was conducted. Gait analysis under dual-task conditions was carried out for all patients. Brain MRI was performed in the absence of contra-indications. Three main gait variables were measured: walking speed, stride frequency, and stride regularity. For each gait variable, the dual task cost was computed and a quartile analysis was obtained. Nonparametric tests were used for all the comparisons (Wilcoxon, Kruskal-Wallis, Fisher or Chi2 tests).
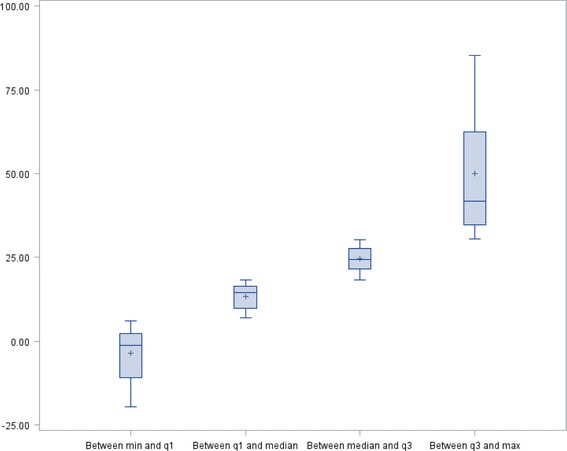
Results: Four clinical subgroups were identified: gait instability (45%), recurrent falls (29%), memory impairment (18%), and cautious gait (8%). The biomechanical severity of these subgroups was ordered according to walking speed and stride regularity under both conditions, from least to most serious as follows: memory impairment, gait instability, recurrent falls, cautious gait (p < 0.01 for walking speed, p = 0.05 for stride regularity). According to the established diagnoses of gait disorders, 5 main pathological subgroups were identified (musculoskeletal diseases (n = 11), vestibular diseases (n = 6), mild cognitive impairment (n = 24), central nervous system pathologies, (n = 51), and without diagnosis (n = 8)). The dual task cost for walking speed, stride frequency and stride regularity were different among these subgroups (p < 0.01). The subgroups mild cognitive impairment and central nervous system pathologies both showed together a higher dual task cost for each variable compared to the other subgroups combined (p = 0.01). The quartile analysis of dual task cost for stride frequency and stride regularity allowed the identification of 3 motor phenotypes (p < 0.01), without any difference for white matter hyperintensities, but with an increased Scheltens score from the first to the third motor phenotype (p = 0.05).
Conclusions: Gait analysis under dual-task conditions in elderly people suffering from gait disorders or memory impairment is of great value in assessing the severity of gait disorders, differentiating between peripheral pathologies and central nervous system pathologies, and identifying motor phenotypes. Correlations between motor phenotypes and brain imaging require further studies.
Keywords: Dual task paradigm; Elderly; Gait analysis; Gait disorders; Motor phenotypes.
Figures
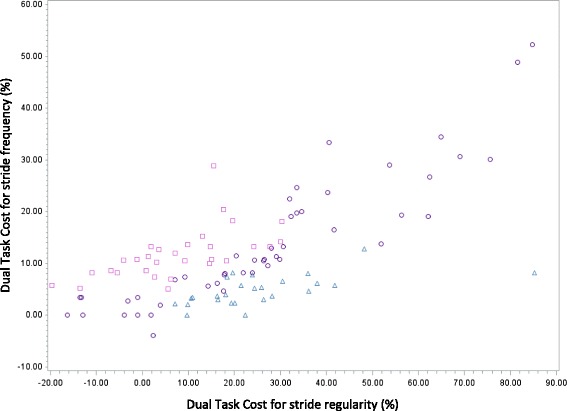
 High value of DTC for Stride Frequency—Low value of DTC for Stride Regularity (n = 30). N°2:
High value of DTC for Stride Frequency—Low value of DTC for Stride Regularity (n = 30). N°2:  Same value of DTC for Stride Frequency and Regularity (n = 47). N°3:
Same value of DTC for Stride Frequency and Regularity (n = 47). N°3:  Low value of DTC for Stride Frequency—High value of DTC for Stride Regularity (n = 26)
Low value of DTC for Stride Frequency—High value of DTC for Stride Regularity (n = 26)References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
