

Acute high-altitude sickness
- PMID: 28143879
- PMCID: PMC9488514
- DOI: 10.1183/16000617.0096-2016
Acute high-altitude sickness
Abstract
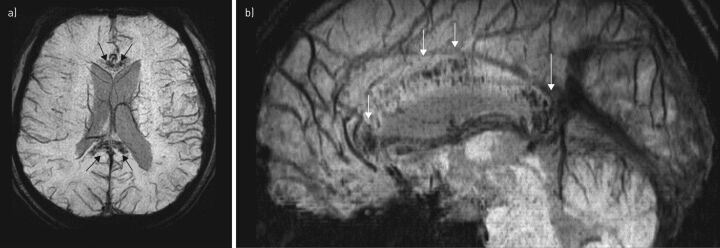
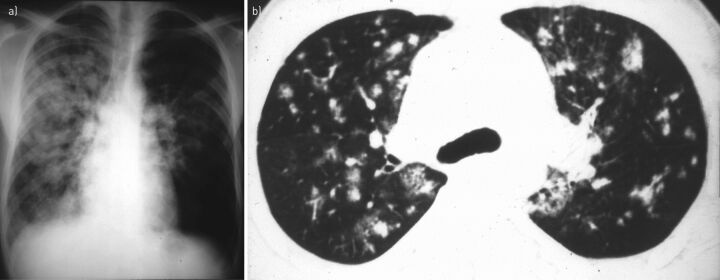
At any point 1-5 days following ascent to altitudes ≥2500 m, individuals are at risk of developing one of three forms of acute altitude illness: acute mountain sickness, a syndrome of nonspecific symptoms including headache, lassitude, dizziness and nausea; high-altitude cerebral oedema, a potentially fatal illness characterised by ataxia, decreased consciousness and characteristic changes on magnetic resonance imaging; and high-altitude pulmonary oedema, a noncardiogenic form of pulmonary oedema resulting from excessive hypoxic pulmonary vasoconstriction which can be fatal if not recognised and treated promptly. This review provides detailed information about each of these important clinical entities. After reviewing the clinical features, epidemiology and current understanding of the pathophysiology of each disorder, we describe the current pharmacological and nonpharmacological approaches to the prevention and treatment of these diseases.
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interests: None declared.
Figures
References
-
- Bartsch P, Bailey DM. Acute mountain sickness and high altitude cerebral oedema. In: Swenson ER, Bartsch P, eds. High Altitude Human Adaptation to Hypoxia. New York, Springer, 2014; pp. 379–404.
-
- Roach RC, Bartsch P, Hackett PH, et al. The Lake Louise acute mountain sickness scoring system. In: Sutton JR, Coates G, Houston CS, eds. Hypoxia and Molecular Medicine: Proceedings of the 8th International Hypoxia Symposium, Lake Louise, Alberta, Canada. Burlington, Vt, Queen City Printers, 1993; pp. 272–274.
-
- Sampson JB, Cymerman A, Burse RL, et al. Procedures for the measurement of acute mountain sickness. Aviat Space Environ Med 1983; 54: 1063–1073. - PubMed
-
- West JB. Con: headache should not be a required symptom for the diagnosis of acute mountain sickness. High Alt Med Biol 2011; 12: 23–25. - PubMed
-
- Wilson MH, Newman S, Imray CH. The cerebral effects of ascent to high altitudes. Lancet Neurol 2009; 8: 175–191. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical