

The Effect of Predialysis Fistula Attempt on Risk of All-Cause and Access-Related Death
- PMID: 28143967
- PMCID: PMC5280018
- DOI: 10.1681/ASN.2016020151
The Effect of Predialysis Fistula Attempt on Risk of All-Cause and Access-Related Death
Abstract
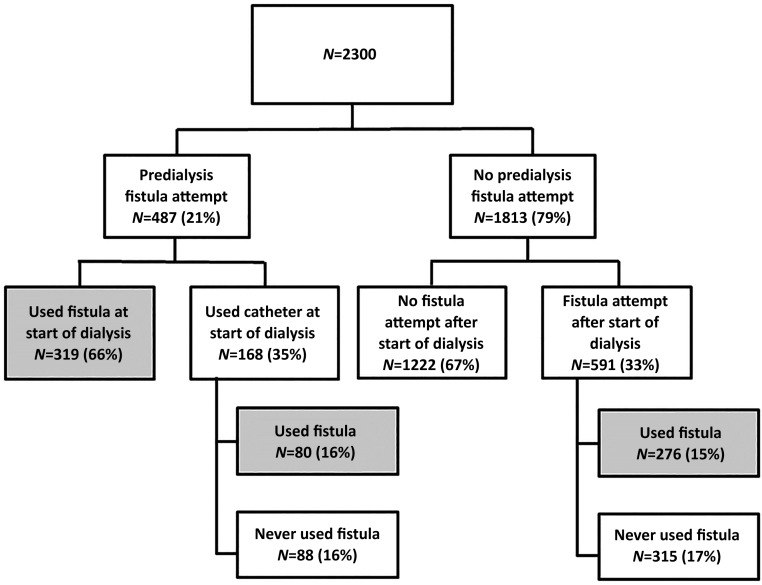
Whether the lower risk of mortality associated with arteriovenous fistula use in hemodialysis patients is due to the avoidance of catheters or if healthier patients are simply more likely to have fistulas placed is unknown. To provide clarification, we determined the proportion of access-related deaths in a retrospective cohort study of patients aged ≥18 years who initiated hemodialysis between 2004 and 2012 at five Canadian dialysis programs. A total of 3168 patients initiated dialysis at the participating centers; 2300 met our inclusion criteria. Two investigators independently adjudicated cause of death using explicit criteria and determined whether a death was access-related. We observed significantly lower mortality in individuals who underwent a predialysis fistula attempt than in those without a predialysis fistula attempt in patients aged <65 years (hazard ratio [HR], 0.49; 95% confidence interval [95% CI], 0.29 to 0.82) and in the first 2 years of follow-up in those aged ≥65 years (HR0-24 months, 0.60; 95% CI, 0.43 to 0.84; HR24+ months, 1.83; 95% CI, 1.25 to 2.67). Sudden deaths that occurred out of hospital accounted for most of the deaths, followed by deaths due to cardiovascular disease and infectious complications. We found only 2.3% of deaths to be access-related. In conclusion, predialysis fistula attempt may associate with a lower risk of mortality. However, the excess mortality observed in patients treated with catheters does not appear to be due to direct, access-related complications but is likely the result of residual confounding, unmeasured comorbidity, or treatment selection bias.
Keywords: arteriovenous fistula; hemodialysis; hemodialysis access.
Copyright © 2017 by the American Society of Nephrology.
Figures



Comment in
-
Vascular Access for Hemodialysis and Value-Based Purchasing for ESRD.J Am Soc Nephrol. 2017 Feb;28(2):395-397. doi: 10.1681/ASN.2016070769. Epub 2016 Oct 6. J Am Soc Nephrol. 2017. PMID: 28143965 Free PMC article. No abstract available.
References
-
- Lee H, Manns B, Taub K, Ghali WA, Dean S, Johnson D, Donaldson C: Cost analysis of ongoing care of patients with end-stage renal disease: the impact of dialysis modality and dialysis access. Am J Kidney Dis 40: 611–622, 2002 - PubMed
-
- Dhingra RK, Young EW, Hulbert-Shearon TE, Leavey SF, Port FK: Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int 60: 1443–1451, 2001 - PubMed
-
- Pastan S, Soucie JM, McClellan WM: Vascular access and increased risk of death among hemodialysis patients. Kidney Int 62: 620–626, 2002 - PubMed
-
- Polkinghorne KR, McDonald SP, Atkins RC, Kerr PG: Vascular access and all-cause mortality: a propensity score analysis. J Am Soc Nephrol 15: 477–486, 2004 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
