

Mechanisms of hypoxemia
- PMID: 28144061
- PMCID: PMC5234199
- DOI: 10.4103/0970-2113.197116
Mechanisms of hypoxemia
Erratum in
-
Erratum: Mechanisms of hypoxemia.Lung India. 2017 Mar-Apr;34(2):220. doi: 10.4103/0970-2113.201292. Lung India. 2017. PMID: 28360486 Free PMC article.
Abstract
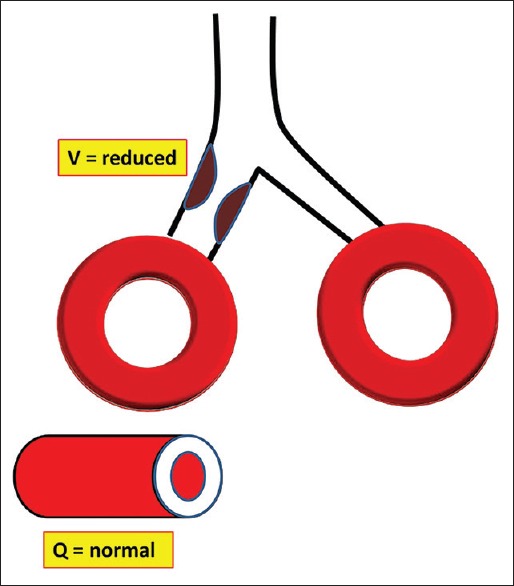
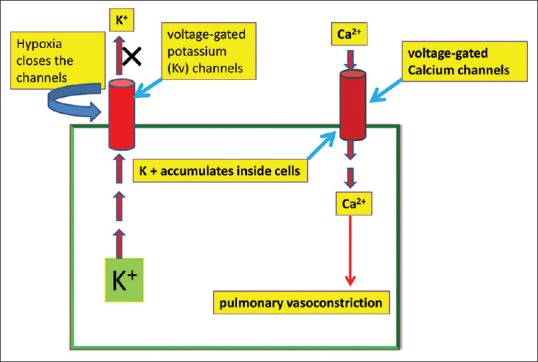
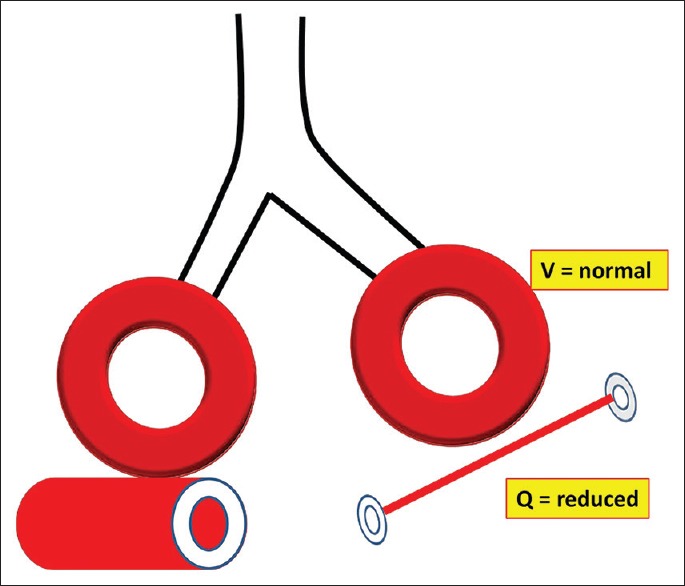
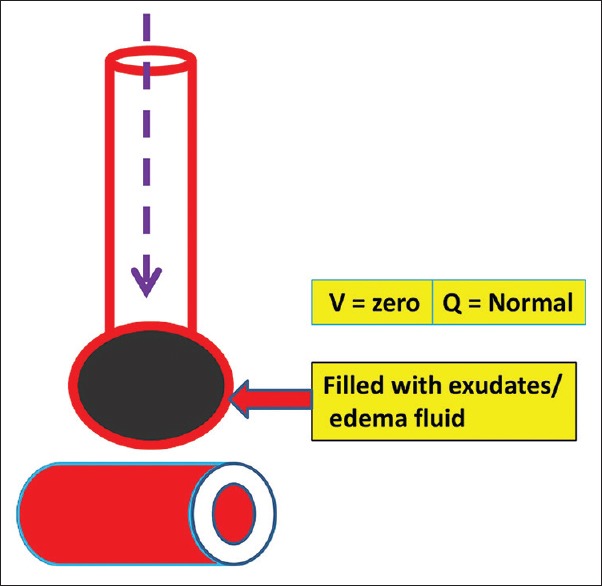
Oxygen is an essential element for life and without oxygen humans can survive for few minutes only. There should be a balance between oxygen demand and delivery in order to maintain homeostasis within the body. The two main organ systems responsible for oxygen delivery in the body and maintaining homeostasis are respiratory and cardiovascular system. Abnormal function of any of these two would lead to the development of hypoxemia and its detrimental consequences. There are various mechanisms of hypoxemia but ventilation/perfusion mismatch is the most common underlying mechanism of hypoxemia. The present review will focus on definition, various causes, mechanisms, and approach of hypoxemia in human.
Keywords: Diffusion limitation; hypoxemia; shunt; ventilation-perfusion mismatch.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Greene KE, Peters JI. Pathophysiology of acute respiratory failure. Clin Chest Med. 1994;15:1–12. - PubMed
-
- Sorbini CA, Grassi V, Solinas E, Muiesan G. Arterial oxygen tension in relation to age in healthy subjects. Respiration. 1968;25:3–13. - PubMed
-
- Belda JF, Soro M, Ferrando C. Pathophysiology of respiratory failure. Trends Anaesth Crit Care. 2013;3:265–9.
-
- Glenny RW. Teaching ventilation/perfusion relationships in the lung. Adv Physiol Educ. 2008;32:192–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
