

Clinical importance of duodenal recesses with special reference to internal hernias
- PMID: 28144266
- PMCID: PMC5206374
- DOI: 10.5114/aoms.2017.64717
Clinical importance of duodenal recesses with special reference to internal hernias
Abstract
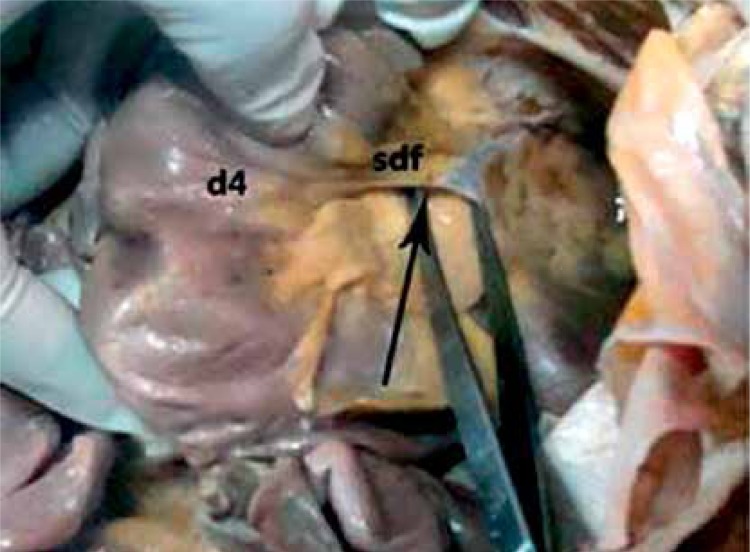
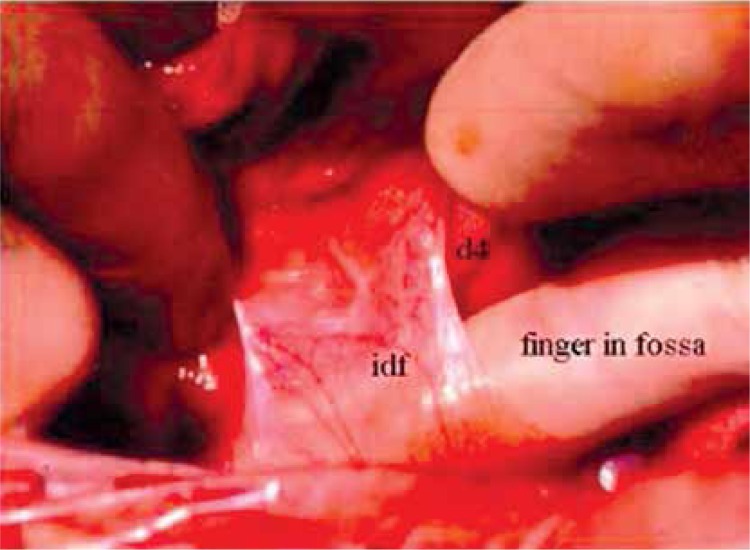
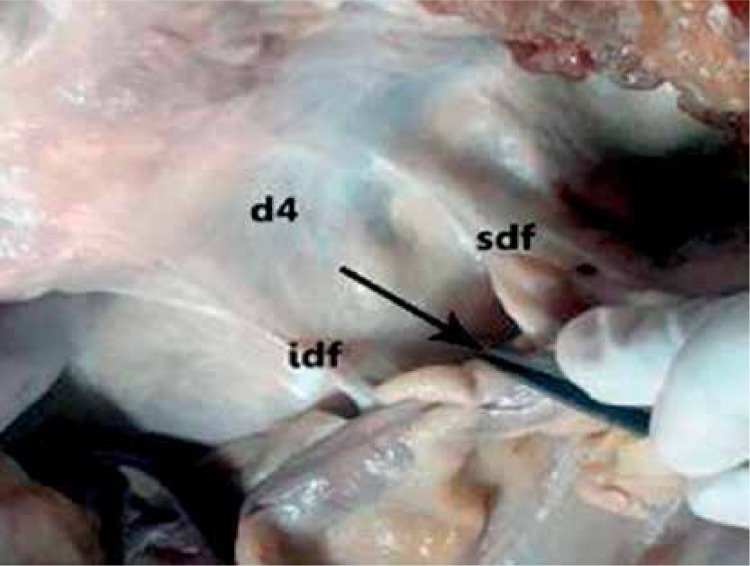
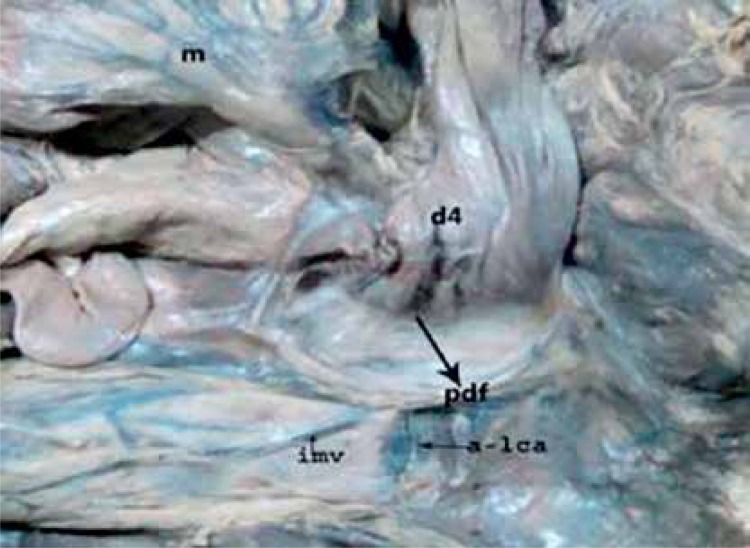
Introduction: The detailed knowledge of the peritoneal recesses has great significance with respect to internal hernias. The recesses are usually related to rotation and adhesion of abdominal viscera to the posterior abdominal wall and/or the presence of retroperitoneal vessels which raises the serosal fold. The duodenal recesses are usually related to the 3rd and 4th parts of the duodenum. Internal hernias with respect to these recesses are difficult to diagnose clinically and usually noticed at the time of laparotomy. So, the knowledge of these recesses can be valuable to abdominal surgeons.
Material and methods: The present study was conducted in 100 cases including 10 cadavers, 45 post mortem cases and 45 cases undergoing laparotomy.
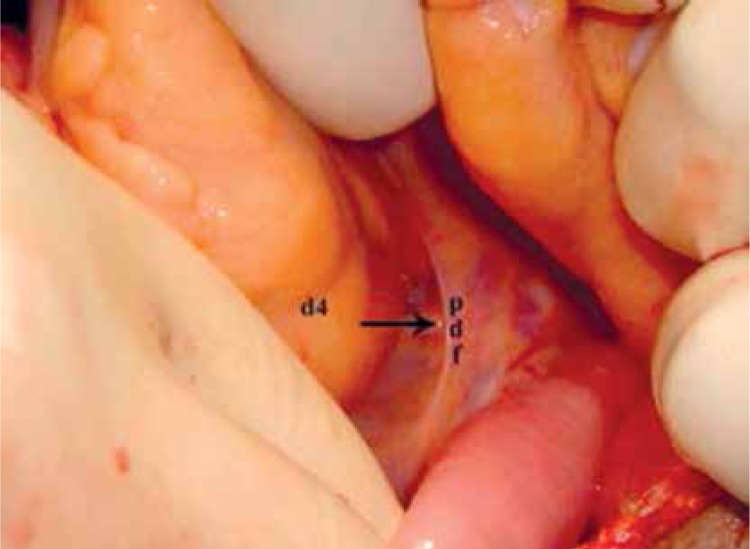
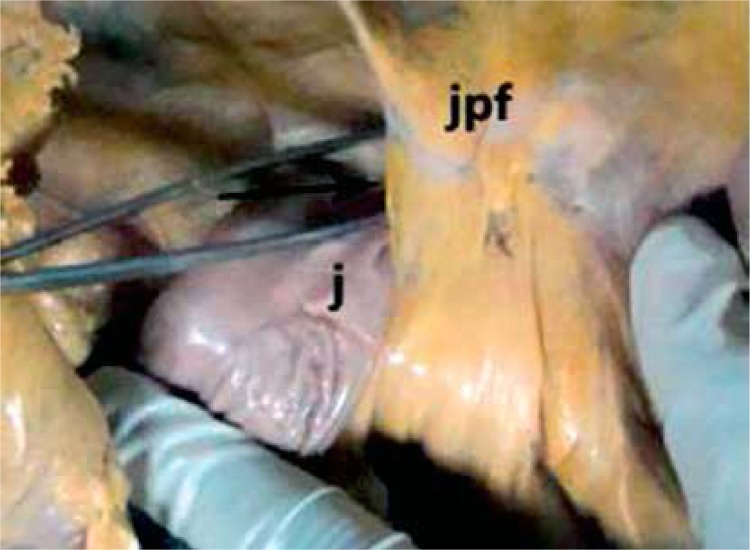
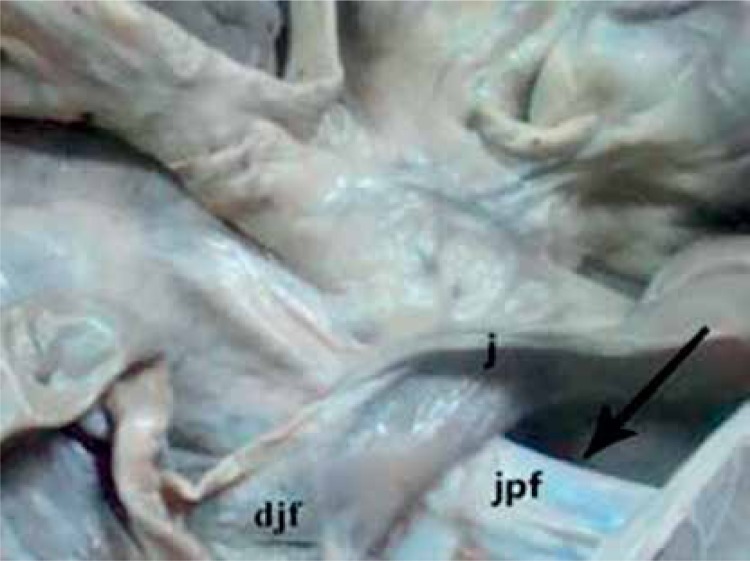
Results: We found superior and inferior duodenal recesses in 28% and 52% respectively, paraduodenal in 12%, mesentericoparietal in 3%, retroduodenal in 2% and duodenojejunal in 18% of cases. Two abnormal duodenojejunal recesses were found, one on the right (instead of the left) of the abdominal aorta, and in the other the opening was directed upwards instead of downwards. The incidence of internal hernias was 3%.
Conclusions: Thus it was observed that there is low incidence of superior and inferior duodenal recesses, and high incidence of paraduodenal recess. The abnormal recesses might be due to malrotation of the gut. In laparotomy cases, the internal hernia was noticed when the abdomen was opened for intestinal obstruction. The incidence of internal hernia was found to be high.
Keywords: internal hernias; peritoneal recesses; retroperitoneal vessels.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Barberini F, Carone VS, Caggiati A, Macchiarelli G, Corner S. An unusual peritoneal fossa: anatomic report and clinical implications. Surg Radiol Anat. 1999;21:287–91. - PubMed
-
- Peltier J, Gars DL, Page C, Yzet T, Launde M. The duodenal fossae: anatomic study and clinical correlations. Surg Radiol Anat. 2005;27:303–7. - PubMed
-
- Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology. 2001;218:68–74. - PubMed
-
- Barberini F, Zani A, Ripani M, Di Nitto V, Brunone F. The complex arrangement of an “aorto-jejunal paraduodenal” fossa, as revealed by dissection of human posterior parietal peritoneum. Ann Anat. 2007;189:299–303. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous