

Intermediate-Risk Chronic Stable Angina: Neutrophil-Lymphocyte Ratio and Fibrinogen Levels Improved Predicting Angiographically-Detected Coronary Artery Disease
- PMID: 28144449
- PMCID: PMC5253433
- DOI: 10.5812/ircmj.18570
Intermediate-Risk Chronic Stable Angina: Neutrophil-Lymphocyte Ratio and Fibrinogen Levels Improved Predicting Angiographically-Detected Coronary Artery Disease
Abstract
Background: Coronary heart disease (CHD) is the leading cause of death worldwide. Research indicates that coronary atherosclerosis is the most frequent cause of CHD. Evidence is scarce concerning the clinical efficacy of fibrinogen or neutrophil-lymphocyte ratio (NLR) measurement in risk-stratifying patients with chronic stable angina.
Objectives: To examine the independent and incremental prognostic value of fibrinogen and neutrophil-lymphocyte ratio (NLR) for angiographically-detected coronary artery disease (CAD).
Patients and methods: In this cross-sectional study, angiography was performed for 183 Iranian patients with chronic stable angina with exercise ECG-determined intermediate risk. Generalized estimated equations were used to obtain the odd ratio (OR) of CAD for a 1-unit increase in log-NLR and a 1-SD increase in plasma fibrinogen. Models were adjusted for established CAD risk factors. Integrated discriminatory improvement index (IDI) and net reclassification improvement index (NRI) were used as measures of predictive ability for CAD, combined with traditional risk factors by NLR and fibrinogen.
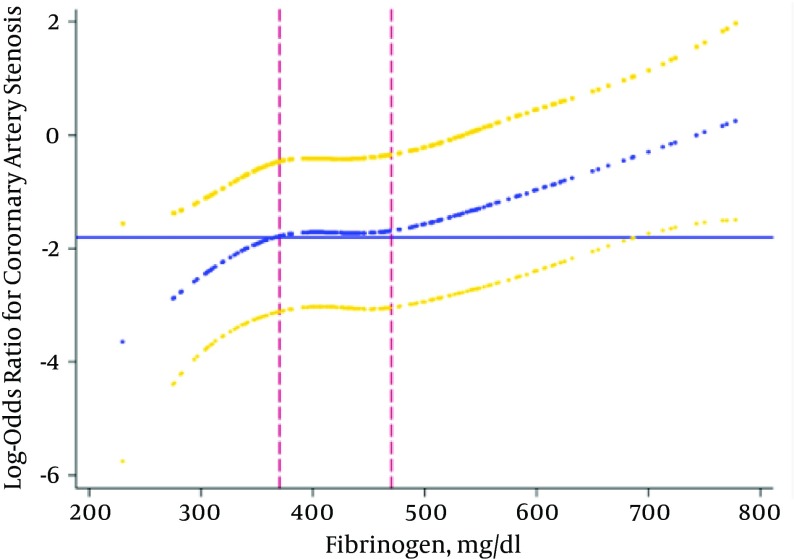
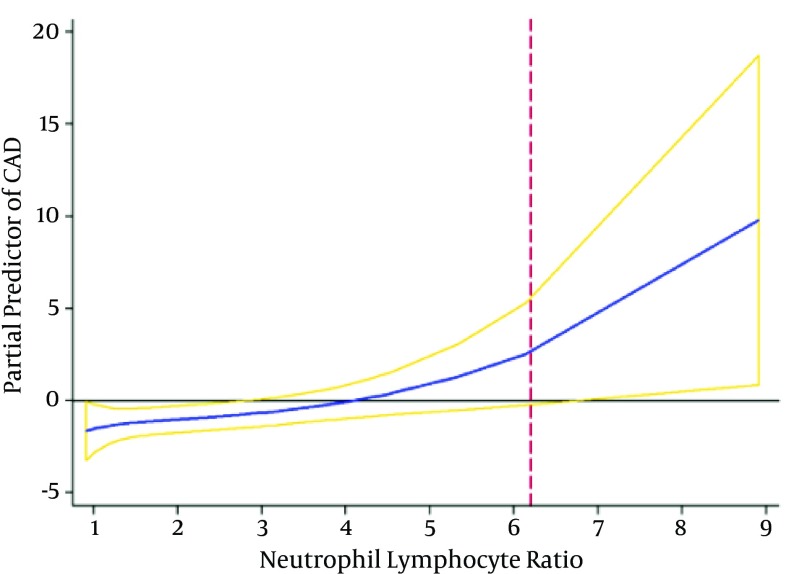
Results: The mean age of the participants was 57.5, with 51.9% being male. Only 12% of participants had angiographically-determined patent coronary arteries. The number of participants with one, two, and three-vessel stenosis were 76, 31, 31, respectively, while 45 did not have stenosed vessels. NLR and fibrinogen levels were significantly higher in patients with stenosis in two (2.4 and 512 mg.dL-1) or three (2.6 and 517 mg.dL-1) coronary arteries, as compared to the group of patients with no significant involvement (2 and 430 mg.dL-1) (all P < 0.01). Patients with a higher NLR and a higher fibrinogen levels were more likely to have higher grades of CAD. OR log-NLR = 1.36 (95% CI: 1.05 - 1.94) and OR Z-Fibrinogen = 1.61 (95% CI: 1.18 - 2.22). When NLR and fibrinogen were added to the traditional risk factors separately, the NRIs were 0.170 (0.023 - 0.324) and 0.380 (0.214 - 0.543), respectively. The NRI was 0.460 (0.303 - 0.620) when both NLR and fibrinogen added to traditional risk factors simultaneously.
Conclusions: NLR and fibrinogen predicted CAD, independent of traditional CAD risk factors. Both measures (whether separately or together) substantially enhanced the predictive performance of traditional risk factors for identifying patients with CAD.
Keywords: Angiography, Atherosclerosis, Fibrinogen, Lymphocyte, Neutrophil.
Figures
Similar articles
-
Neutrophil lymphocyte ratio significantly improves the Framingham risk score in prediction of coronary heart disease mortality: insights from the National Health and Nutrition Examination Survey-III.Int J Cardiol. 2014 Feb 15;171(3):390-7. doi: 10.1016/j.ijcard.2013.12.019. Epub 2013 Dec 23. Int J Cardiol. 2014. PMID: 24388541
-
Incremental diagnostic value of circulating pentraxin in patients with intermediate risk of coronary artery disease.Heart. 2013 May;99(9):640-8. doi: 10.1136/heartjnl-2012-303560. Epub 2013 Mar 6. Heart. 2013. PMID: 23468517
-
Pre-procedural neutrophil-to-lymphocyte ratio and long-term cardiac outcomes after percutaneous coronary intervention for stable coronary artery disease.Atherosclerosis. 2017 Oct;265:35-40. doi: 10.1016/j.atherosclerosis.2017.08.007. Epub 2017 Aug 18. Atherosclerosis. 2017. PMID: 28843126
-
The Combined Impact of Neutrophil-to-Lymphocyte Ratio and Type 2 Diabetic Mellitus on Significant Coronary Artery Disease and Carotid Artery Atherosclerosis.J Cardiovasc Ultrasound. 2016 Jun;24(2):115-22. doi: 10.4250/jcu.2016.24.2.115. Epub 2016 Jun 22. J Cardiovasc Ultrasound. 2016. PMID: 27358703 Free PMC article.
-
Prognostic value of the neutrophil to lymphocyte ratio for cardiovascular diseases: research progress.Am J Transl Res. 2025 Feb 15;17(2):1170-1177. doi: 10.62347/KVCV7377. eCollection 2025. Am J Transl Res. 2025. PMID: 40092102 Free PMC article. Review.
Cited by
-
Association between neutrophil-lymphocyte ratio and arterial stiffness in patients with acute coronary syndrome.Biosci Rep. 2019 May 3;39(5):BSR20190015. doi: 10.1042/BSR20190015. Print 2019 May 31. Biosci Rep. 2019. PMID: 30992389 Free PMC article. Clinical Trial.
References
-
- McGovern PG, Pankow JS, Shahar E, Doliszny KM, Folsom AR, Blackburn H, et al. Recent trends in acute coronary heart disease--mortality, morbidity, medical care, and risk factors. The Minnesota Heart Survey Investigators. N Engl J Med. 1996;334(14):884–90. doi: 10.1056/NEJM199604043341403. - DOI - PubMed
-
- Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation. 1995;92(3):657–71. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous